
Effective teamwork in interprofessional healthcare teams requires expert performance by individuals in clearly defined roles. This focus on role clarity and role performance provides the basis of the ‘pit crew’ approach, now commonly utilized in resuscitation teams with demonstrated benefits in patient care. Maternity teams responding to emergencies may benefit from a similar approach to teamwork; however, little attention has been paid to team member roles within the maternity emergency context. In this qualitative case study of maternity teams responding to two simulated maternity emergencies in the context of a teamwork training course, we aimed to describe team member performance in roles and explore clinician perceptions of role allocation and performance within the team. Video analysis of role performance demonstrated team members performed actively and passively in multiple roles throughout the scenario, with some improvement in role consistency between Case 1 and Case 2. Workload distribution was uneven, with some clinicians performing tasks across several roles concurrently, while others did not appear to take on any role. Thematic analysis of debriefing conversations and post-scenario interviews and focus groups revealed four themes. Three themes related to the process of team member allocation to roles with participants describing the need to firstly gain an understanding of the situation, have knowledge of clinical requirements and priorities and consider their suitability for role in the clinical case. The fourth theme related to participants shift in conceptual understanding of how to work in roles facilitated by the simulations and debriefings. This study provides a preliminary understanding of how team members allocate roles in ad hoc maternity teams and supports the use of simulation-based training to improve role-based teamwork. Further research is recommended to enhance our understanding of the impact of role-based teamwork in maternity emergencies, and how simulation and debriefing can most effectively improve this important domain of teamwork.
Due to the critical importance of teamwork in healthcare emergencies, simulation-based training is widely recommended to improve outcomes [1,2]. A key element of effective teamwork is team members’ allocation to, knowledge of and performance in team roles which is a common item of assessment in teamwork assessment tools [3–5]. The inclusion of these elements in such tools indicates the importance of role allocation, which simulation programs should focus on when teaching and improving team function. Yet, what these roles are, to our knowledge, have not been clearly defined in the literature and therefore empiric evidence for roles in maternity emergencies is lacking. Developing a commonly understood and utilized team model is a key step in developing a curriculum for teamwork training, and defining those team roles is arguably an important part of any team model [6].
While the theoretical benefits of clearly defined team roles have been established in the teamwork literature [7], there has been surprisingly little attention paid to role definition in the medical emergency team research. One reason for this could be the heterogeneity of team structures within healthcare. Some interprofessional team members may have their roles determined by their professional background, and the tasks within that role are clear due to a specific scope of practice for that profession. As an example, a surgical team consists of several team members whose roles, and tasks within each role, are defined by their professional background or seniority. In a surgical team, the surgeon, surgical assistant, anaesthetist, anaesthetic assistant, scrub and scout midwife would rarely become confused about who was doing what task, in both routine and non-routine work in the operating room.
Other teams, particularly ad hoc teams, require a different structure. Compared to surgical teams, ward resuscitation teams are far less organized, albeit in their early formation. As a way of dealing with this issue, Basic life support (BLS) training programs have overcome the problem of the ad hoc team by defining roles by time of arrival – first responder, second responder, third responder and so on, each with specific tasks for each role. In this way, even if all three initial responders are of the same professional background, the task expectations are clear, and the team members can execute the expected tasks without requiring explicit direction. Other teams which include groups from the same profession may pre-allocate roles and make these explicit through role tagging [8,9].
Describing team member roles and the tasks within each role is a key feature of a horizontal resuscitation approach [10]. This approach, often referred to as the ‘pit crew’ model, has been adopted in many resuscitation teams with positive effects on care delivery [11,12].
Team members in each allocated role perform specific tasks independently without requiring instruction from a leader [13]. Tasks within roles may have interdependencies with other roles; hence, understanding of other team members roles and tasks within a role requires a degree of co-ordination. Co-ordination commonly occurs through a team leader (or leaders); however, when there is mutual understanding of each other’s roles, which can be enhanced by cross-training, teams can function effectively with less directive leadership via implicit co-ordination [14]. Additional gains in team performance occur when team members are able to act beyond their roles through mutual performance monitoring and back up behaviours [15].
With perhaps the exception of the accoucheur or team leader, many members of a team responding to a maternity emergency do not typically have a priori knowledge of the potential roles they might take on and the specific tasks expected within these roles. Accordingly, maternity team training has often attempted to overcome this challenge by training directive leaders who allocate tasks to team members, rather than taking a role-based approach. However, maternity team leaders may become overloaded overseeing both the clinical and logistical management of the situation [16]. While healthcare emergency teams that have adopted a pit crew approach demonstrate improvements in team performance [11,12], the feasibility and acceptability of a similar approach in the maternity setting are uncertain.
The aim of the paper is to describe maternity team members’ performance in specific roles during emergency response. By employing a case study approach, the second aim is to explore the learning and development of clinician’s understanding of role allocation during simulation-based training. By gaining a deeper understanding of the phenomenon of how they perform in and learn about role allocation within maternity emergencies, this study will provide important information to inform development of team management and teamwork training in maternity care.
A case study approach was designed to develop the understanding of how clinicians learn and perform role allocation within maternity emergency response teams. The approach aims for an in-depth exploration from multiple perspectives of the focused phenomena in real-life context [17]. In the method, cases are bounded by time and activity, and researchers collect detailed information using a variety of data collection procedures over a period of time [18].
It is important that case studies employ a triangulation process to develop a holistic understanding of the focused phenomena [19]. Within the methodological framework, this study employed multimethod data collection to collect field documentations, observations of simulation and debriefing, and post-debriefing interviews. These data were then analysed through different methods (i.e. video analysis, thematic analysis) to provide in-depth evidence for participants’ learning and development of understanding role performance [17].
The study was conducted at a simulation centre co-located with a tertiary maternity unit in Queensland, Australia. Healthcare staff and students working in the hospital were the participants. They attended an 8-hour interprofessional team training course for maternity care clinicians with a focus on teamwork and clinical skills. Clinicians attending the workshop included anaesthetic and obstetric doctors, midwives, and student midwives: all with various levels of clinical experience, replicating the skill mix in the work environment.
The workshop involved six immersive simulations, each followed by a facilitated team debriefing. Two debriefers, both obstetric and midwifery educators, had undertaken debriefing training in the use of the debriefing with good judgment approach [20]. In addition to the immersive simulations, interactive lectures and hands-on activities were embedded throughout the day. Participants were invited to participate in the research component of the course, but the content and delivery were not altered due to the research.
The workshop was conducted in September 2018. The data were collected as part of a larger project focusing on cross-sector simulation-debriefing [21]. The unique data involved in this present study were snapshots of two simulation-debriefing sessions. These simulation-debriefing sessions were selected to explore the concept of role allocation, which was highlighted as an area of inquiry earlier in the project [21]. Case 1 was the second scenario of the day, with Case 2 being the sixth and final scenario. The two cases were selected by the research team for detailed analysis as it was anticipated to demonstrate, by comparing these cases, the learning and development of participants’ understanding role allocation and how team performance improved throughout the day. Details of the simulation scenarios examined for the research were outlined in the next section.
The model of maternity team role allocation (Table 1; Figure 1) was presented to the participants after the first scenario of the day, prior to Case 1. The model was informed by the group’s clinical expertise in maternity care, discussions with clinical experts in emergency and trauma care and descriptions of pit crew models within the healthcare literature [9,10,22]. The model was developed by the first author’s institutional simulation training faculty group and has been adapted for use in other institutions [23].

| Role and ideal position | Assessment tasks | Management tasks (as required) | Ideal position |
|---|---|---|---|
| Team leader | • Ensure team roles allocated • Oversee clinical assessment and management plan • Ensure team informed with recaps • Ensure communication with external agents |
Foot of bed | |
| Airway | • Level of consciousness • Airway patency • Breathing and oxygenation |
• Communicate with woman on behalf of team • Protect airway • Apply oxygen |
Head of bed |
| Circulation a | • Pulse, blood pressure, oxygen saturation | • Prepare for or insert intravenous lines • Collect bloods • Initiate fluid resuscitation |
Chest level – side of observations machine |
| Drugs a | • Current infusions • Recent drugs given |
• Stop or commence infusions • Prepare and administer drugs |
Chest level – side of infusion pumps |
| Abdomen | • Fetal heart monitoring • Uterine tone, contractions, fundal height • Other abdominal assessment |
• Suprapubic pressure (shoulder dystocia) • Fundal massage |
Level of abdomen |
| Pelvis | • Loss – amount/type • Speculum or vaginal examination • Trauma |
• Apply fetal scalp electrode (FSE) • Deliver baby/placenta • Address bleeding trauma • Insert in dwelling catheter |
Between legs or at knee level |
| Scribe | • Document on appropriate clinical form • Use form as a cognitive aid to guide team assessment and management. • Ensure incident logged when required |
Adjacent to team leader |
aRoles may not be required in shoulder dystocia – can assist with external manoeuvres.

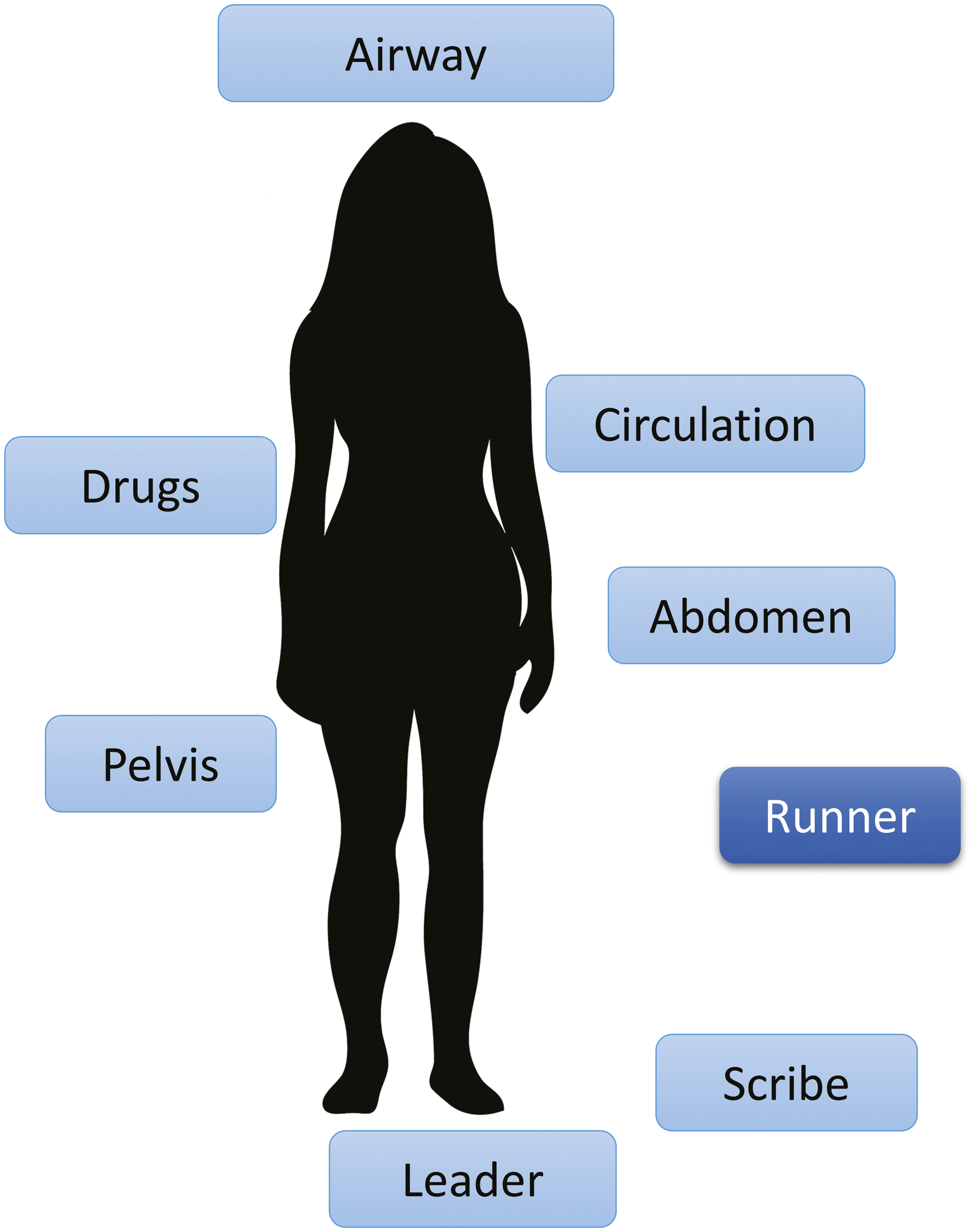
Maternity team model.
Following Case 1, the participants either observed or participated in three further simulation scenarios prior to Case 2, allowing for continued rehearsal and improvement of role allocation within the team response to the emergency.
All activities (scenario simulations and debriefings) were video-recorded, and the debriefings and post-debriefing interviews were transcribed for further analysis. In order to record the experiences of all participants, four out of five researchers interviewed participants individually while one researcher interviewed the remaining participants in a focus group format (see Supplementary Appendix 1). Therefore, all participants had opportunities to discuss their experiences with simulation and debriefing sessions. These reflective interviews were focused on positive and negative aspects of their learning experiences and lasted approximately for 10 minutes. Based on the researchers’ reflections, the extra question was added for the Case 2 interview to ask the participants to describe the steps of allocating a role to themselves when entering in a simulation room.
Within the case study design, the variety of data sources were analysed to provide different perspectives to develop a holistic understanding of how the participants perform role allocation and improve their role performance. All data were analysed for their specific purposes: (1) video analysis of simulations for behavioural observation, (2) thematic analysis of debriefing transcriptions for team’s learning and reflection and (3) thematic analysis of post-simulation interviews for individual reflection and learning.
First, to investigate how the participants performed role allocation, the research team conducted video analysis of simulated performance using the maternity team model previously developed by the simulation team. The maternity team model was used to define eight roles common in maternity emergencies (see Figure 1). However, an adaptation of the model was necessary for Case 2 where the scenario also required BLS (see the Results section). The second form of analysis was thematic analysis of two different data sources (debriefing and interviewing texts), focusing on their understanding of role allocation from team and individual reflections [24]. All data were imported into an NVivo project (QSR) for the analysis, and the outcomes of these analyses were synthesized.
Video analysis has a long history to analyse human behaviour [25] and was highlighted in a special issue of Qualitative Research in 2012 [26]. Moreover, video analysis has been used in two different approaches for industrial research. First, video recording was used as a tool for participants to reflect on their own performance in aviation [27] and construction industry [28]. Second, video analysis was used by non-video participants (i.e. researchers) for purpose of a specific research focus [29].
In this study, video analysis was interpretative rather than standardized: That is, rather than focusing on validating the code by tests on inter-coder reliability, it aimed to complement the holistic understanding of how the participants learn role performance through thematic analysis with objective evaluation and close analysis of the video footages (i.e. overall descriptive analysis and interactions among the team members).
Each video of simulation scenario was divided into 5-second segments in NVivo. Each segment was then coded first by YK and TJM for each participant, relevant to the role they were performing at that time. This determination was based on the geographic position (see Figure 1) of the team member and any observed tasks performed relevant to the role (see Table 1). The same activity was repeated by YK and SJ to confirm the codes. Participants in roles were then scored as a ‘2’ if actively performing tasks relating to a role. They were scored as a ‘1’ if they were not active but monitoring a role position. They were scored a ‘0’ if could not be identified a participant was in a role. Participants identified as doing more than one role in a 5-second segments were score for both. That is, scores above 2 were recorded occasionally.
After coding, the NVivo transcriptions were exported into Microsoft Excel spreadsheet, cleaned and calculated for performance scores assigned to role-related activity. Individual scores were pooled to demonstrate overall role activity in each simulation (Figure 2) and for each participant (Figure 3). Finally, a matrix representing the intensity of role tasks performed by the team members for the duration of each case was produced (Figure 4).
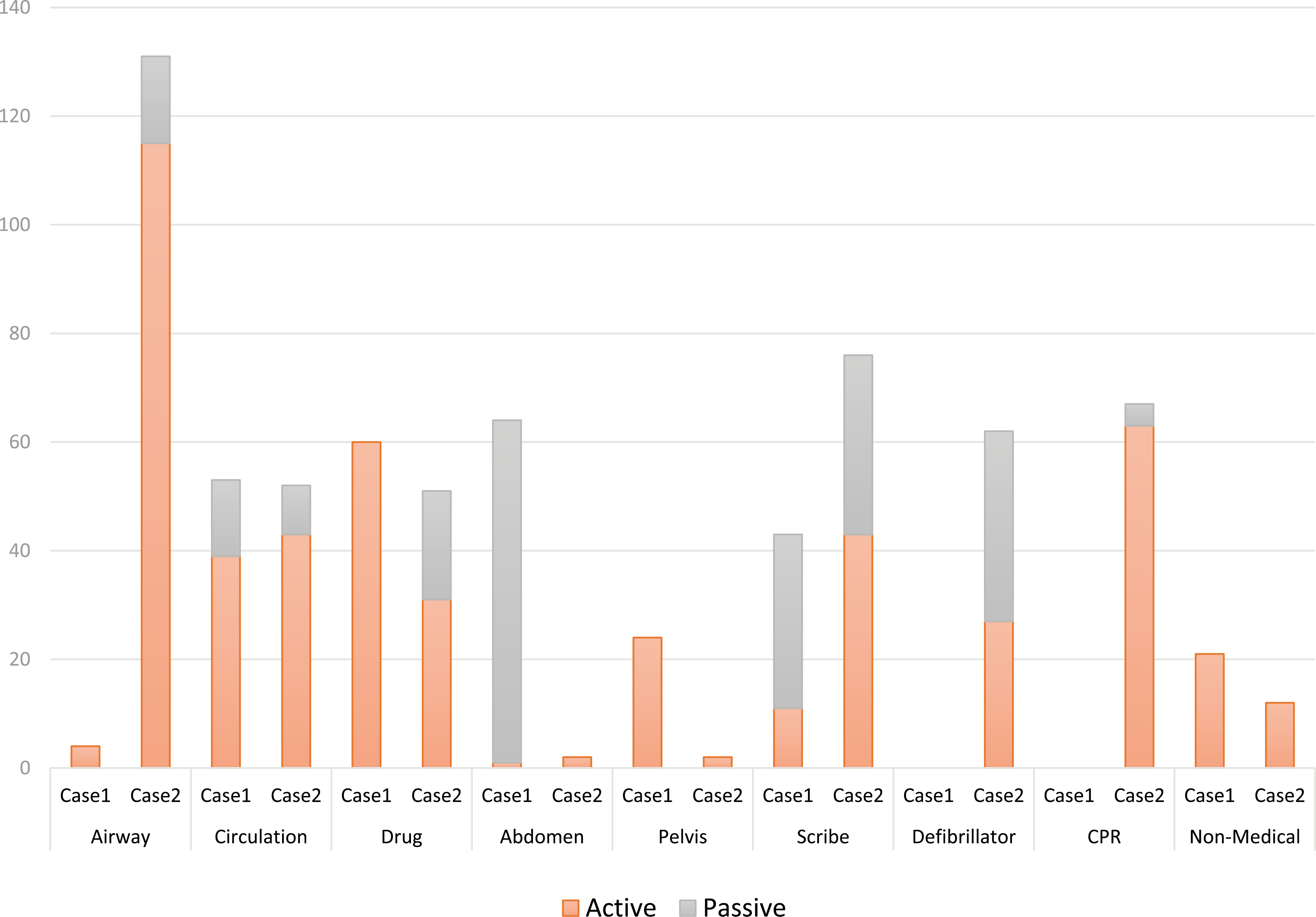
Role-related activity: Case 1 and Case 2
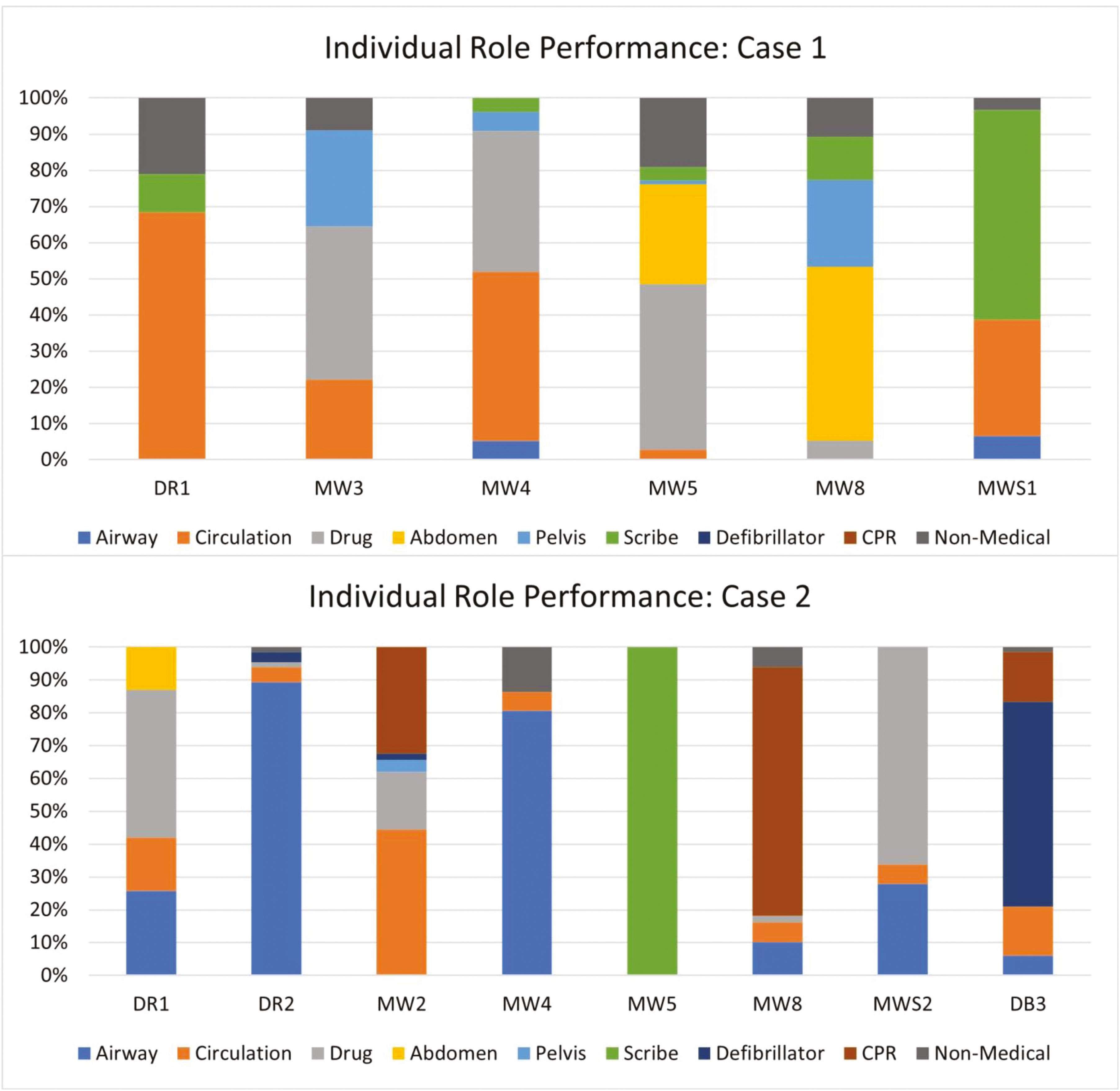
Individual role performance.
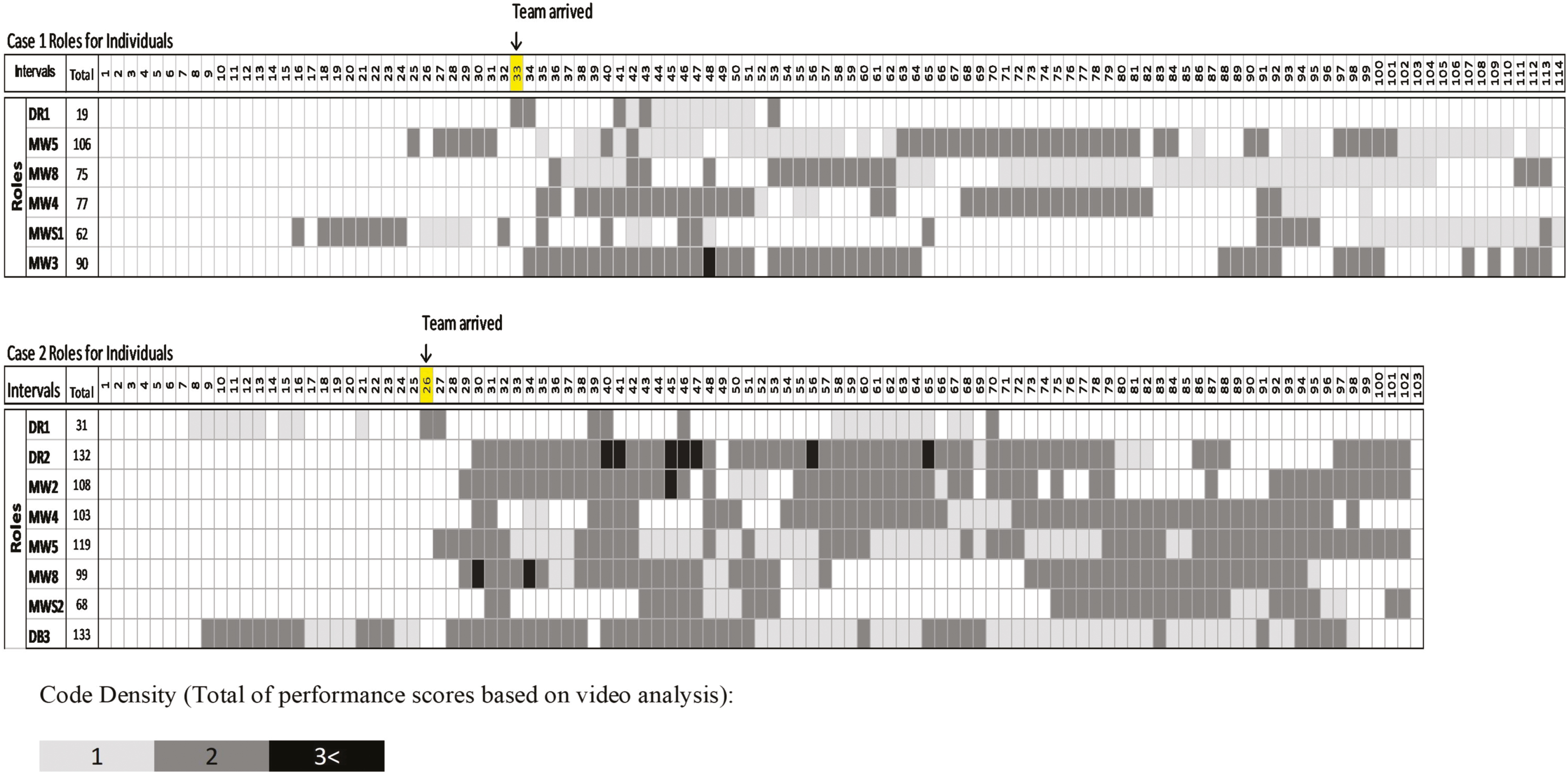
Team role performance.
Thematic analysis was used to analyse transcribed texts of team conversations during debriefing and interviews [24]. First, SJ and YK read through both texts carefully and then discussed key concepts of ‘learning and process of role allocation’. The 33 separate concepts were initially found and coded to single nodes in NVivo. These nodes were then inspected for its meaning and grouped into more meaningful nodes. A total of four themes were identified.
Thirteen clinicians participated in the research course. They all either participated in or observed scenarios throughout the day, and all participants (active in the simulation or observing) participated in the post simulation debrief (see Supplementary Appendix 2 for the further details of participants, their simulation participation and interview formats).
Case 1 and Case 2 scenarios are summarized in Table 2.
| Case 1 (9 minutes 33 seconds) | Case 2 (8 minutes 55 seconds) |
|---|---|
| A senior midwife (MW5) and midwifery student (MWS1) took over the care of a woman in labour. The woman was found to be mildly hypertensive and progresses rapidly to an eclamptic seizure. A team of four additional staff (two midwives, an obstetric registrar and resident) entered the room in response to the call for help. Immediate assessment and management of the seizure occurred. A fetal bradycardia begun during the seizure which resolved after the seizure ended. The team made a plan for ongoing care. The debriefing followed immediately after the scenario completion and lasted for 29 minutes 13 seconds. | An obstetric registrar (DR1) was called by an embedded simulation participant (ESP) midwife (DB3) to review a postnatal patient on the birth unit who had developed shortness of breath after a vaginal delivery. The woman was hypoxic and as more help was called for, she became unresponsive. Basic life support was instituted, and the arrival of the emergency team (anaesthetist, obstetric resident and four additional midwives) saw a shockable rhythm detected and managed. A differential diagnosis was worked through and a plan for ongoing care was developed. The debriefing lasted for 24 minutes 40 seconds. |
Figure 2 shows the overall results from analysing role performance of all team members in Case 1 and Case 2. Consistent with the different scenario types, two additional roles were required in Case 2 (compression and defibrillation) and there were fewer tasks performed related to abdomen and pelvis roles compared to Case 1. There was less participation in the airway role in the Case 1, compared to Case 2, in which the patient required intubation and ventilation rather than basic airway support.
In both Case 1 and Case 2, no team member took a hands-off leadership role and there was no verbal declaration of leadership assignment during the scenarios; therefore, ‘leader’ was coded as ‘0’. Those who assumed implicit leadership during the scenario were actively involved in other role tasks concurrently.
Figure 3 presents the stacked bar charts from the analysis of each case. Overall, less switching between different roles were observed in Case 2 compared to those in the Case 1. For example, MW5 performed five tasks across five different roles in Case 1 including Circulation, Drugs, Abdomen, Scribe and Non-Medical tasks but performed in only one role (Scribe) in Case 2.
Figure 4 shows the code density based on individual participants’ engagement in roles-related tasks (either passive or active). Overall, lighter shades in the Case 1 matrix suggested less engagement in roles, compared to a greater number of darker shades in the Case 2 matrix. This is consistent with the confirmed different complexity experienced between the two scenarios: Case 2 involved more tasks and roles, and clinicians were more likely to be required to be active in those roles when compared to delivering the care required in Case 1.
This analysis also revealed the degree of workload distribution among team members. For example, there were moments in both cases, where some team members were heavily engaged in role-related tasks, and two or more other team members were not performing any role, even in a passive state (e.g. scored as 1; Case 1 segments 65–112; Case 2 segment 54–73). DR2 (Anaesthesia) in Case 2 did not only consistently engage in a role throughout the scenario but also undertook multiple tasks across different roles occasionally. The close video observation also revealed that he took an implicit primary leadership role. In contrast, when DR2 was performing tasks in multiple roles (segments marked black) other team members (in particular DR1) were not engaged (either passively or actively) in any specific roles, suggesting a maldistribution of workload.
Thematic analysis of debriefing and interview texts identified four themes relating to role-related performance: (1) understanding the situation, (2) prioritizing and knowing what needs to be done, (3) suitability of a role and (4) conceptual shift in understanding role allocation.
The participants’ discussions outlined importance of understanding what was happening in the emergency situation for the team to effectively organize themselves into roles. Having a clear understanding of what was happening appeared to be a critical first step in team organization. They emphasized the importance of effective leadership and clear communication, including sharing situational information through handovers and recaps in understanding the situation.
In particular, the participants became comfortable to verbalize what they were doing, or what they were and were not capable of:
At the beginning, I didn’t feel the confidence to [speak up], and I think that as the days progressed, the importance of people talking and saying what they’re doing has just [being emphasised.] You’re not telling anyone what you’re doing, [That] is not helpful. (MWS2 in CASE2 Interview)
The participants expressed increased feelings of control between Case 1 and Case 2 simulation. Following Case 1, feelings of uncertainty in understanding the situation inhibited their ability to effectively allocate roles.
I thought that everybody knew they needed that role allocation, and were trying to allocate, but for me from my perspective, weren’t really sure what was going on, where you were wanting to try and get yourself a role, but I was completely lost in the scenario. (MWS2 in CASE1 Debrief)
They expressed that working in roles helped them reduce a feeling of chaos and gain greater understanding, even though they might not yet have a clear diagnosis.
The first situation… I feel like it was chaos, and everyone kept saying it was chaos it was chaos.... Whereas in the last scenario where they still at the end were still like “So what was it?” But everyone said but it wasn’t chaotic…. You still might be confused and be like “I’m not sure.” But we still have done all the roles, and the person is stable because we all know what to do. (MW6 in CASE2 Interview)
Furthermore, doctors and senior midwives discussed the importance of understanding what was required of the situation through effective leadership to organize the team. In Case 1, when there was confusion regarding patient assessment, DR1 recapped frequently and sought information from team members who were performing tasks while switching across various roles. In contrast, very early in Case 2, DR2 verbalized the problem (cardiac arrest) which led the team to quickly fill in the roles required for the situation, the differences are illustrated in Figures 3 and 4.
Leadership was not announced during the simulations but discussed as important in role allocation.
It did appear that everyone sort of found their role and yeah, I think that was largely due to DR1’s leadership. (MW6 CASE1 Interview)
Furthermore, the senior midwife (MW5), acting as scribe in Case 2 appeared to act as a secondary leader, directing others and seeking information from team members, including from DR2 who appeared to assume implicit medical leadership. This was in keeping with reflective comments in the debriefing of Case 1 about the scribe being a senior midwife who should also take on a leadership role, outlined in theme 4 below.
This theme revealed the importance of participants understanding what roles were needed and the role priorities. Without this knowledge they find it hard to take on a role.
Maternal collapse, my knowledge of drugs that are needed or actual steps to do is not there. So it’s harder to feel useful (MWS2 Case1 Interview)
In contrast to junior clinicians, doctors and experienced midwives talked about the process of finding role tasks based on their prior experiences and knowledge.
For me whatever needs to be taken care of first and then I go to it and then someone more experienced in that area comes…and you go to the next most needed thing that needs to be done (MW2 CASE2 Interview)
I always gravitated towards the things that I’ve done in clinical setting before…I think I gravitated towards things I was more comfortable in. (MW7 in CASE2 Focus Group)
By understanding the clinical roles, and the priorities of those roles, allowed doctors and senior midwives to naturally assess which roles were most important at that time.
This theme represents the individual role suitability that the participants considered when allocating a role to themselves or team members. For example, the team discussed the role of airway is assigned to someone certified for intubation and scribe is allocated to a more experienced team member. Much of the debriefing conversation following Case 1 focused on the role of scribe: Who should or should not be assigned that role, and how to develop skills in scribing during emergencies. Figure 3 showed that three novice midwives took turns as scribe in Case 1. A student midwife expressed her concerns about inexperienced clinicians taking a role as a scribe:
As a student doing emergency documentation, …somebody is going to have co-sign that. And obviously if things went terribly wrong, that’s the actual legal documentation somebody’s going to have. (MWS1 in CASE1 Debriefing)
Other staff agreed that more senior staff should take the scribe role, and this person should be capable of filling in a leadership role.
Documentation needs to be a more senior.… It’s important because that person can do the recap, that person can take the secondary lead position, that person can direct other people to do other things because she’s got it right there what’s already happened. (MW 3 CASE1 Interview)
It was also considered important to be comfortable in a role, or conversely speak up if not.
I think it’s really good that people should get [a role] they’re comfortable doing. And they actually step up and do what they’re comfortable with and stay with it, in that role. (DR2 in CASE2 Focus Group)
This example was demonstrated in the Case 2 video observation where MWS2 opened a bag of intubation equipment but then asked MW4 to complete the role of assisting DR2’s intubation.
Participants described the process of debriefing in changing their perceptions of role allocation in ways consistent with results seen in the video analysis. In Case 1 debriefing and interviews, participants expressed guilt or discomfort when having no role to perform, and they actively walked around looking for a role. In Case 2 debriefing and interviews, however, participants expressed acceptance of staying at the same role even though not actively performing a role-related task.
…not trying to do more than one task at a time, but like just going to stick with what you’re doing and do it well…especially if you are doing something like leading and documenting, just keep doing that and find the other people that can do [other tasks]… that you don’t need to be distracted by. (MW6 in CASE2 Debriefing)
This finding was consistent with the video analysis showing participants changing roles frequently in Case 1, while maintaining a more static role in Case 2 (Figure 3).
It felt really calm, and it felt like people weren’t looking for anything to do, like in a good way rather than “I have no idea what to do”. So that’s what it looked like to me. (DB2 in CASE2 Debriefing)
The maternity team model appeared to provide a clear understanding of what needs to be done which contributed to the conceptual shift and improve the overall team performance.
...more emphasis on the individual roles was very helpful…because I kind of knew all those roles were there. But…the importance of each person’s role was emphasised more. So that was actually probably a moment that I sort of, I’ll take that with me. (MW1 in CASE2 Interview)
In reflecting upon their own perceptual shift, participants highlighted the need for others to share the same understanding for the maternity team model to be effective in the clinical environment.
You run through your basic [clinical] stuff when you orientate, but this sort of stuff, with that team and role allocation, you don’t get refreshed on that…. We could standardise it so that everyone’s got that basic understanding of role allocation and things, like everyone participates in, like even with emergencies. (MW7 in CASE2 Debriefing)
The theme 4 highlights how participants changed or deepened their understanding of role allocation in emergencies and began to consider ways in which to apply this new model in the clinical environment.
This paper presents novel data regarding clinicians understanding of and performance in, roles in a maternity emergency response team. The case study demonstrated perceived improvements in team members allocation to and consistency in role performance between Case 1 and Case 2. Fundamentally, the findings of this study identify role allocation to be contingent on understanding the situation, knowledge of roles and their priorities, and self-perceived suitability for the role. The study findings also support the role of simulation and debriefing in changing participants understanding and perceptions of working in a role-based approach to teamwork (see the figure of overall findings in Supplementary Appendix 3).
The need for teams to first understand the situation through clear communication to rapidly allocate and perform in team roles may be one reason why teams that use techniques to enhance a shared mental model have better clinical performance [30,31]. As an example, Siassakos et al. [30] noted that teams with an earlier and clearer verbal declaration of the nature of the emergency were able to deliver a critical medication sooner than teams who did not. Other studies have highlighted behaviours such as talking to the room and providing frequent situational updates as key markers in high-performing teams [32,33]. While these studies have not specifically investigated the relationship between these behaviours and role-related performance, it is plausible that effective role performance is one mediator of this relationship, particularly in maternity teams where members frequently arrive at an emergency without a briefing on the nature of the situation or pre-allocated roles.
This study has also highlighted the challenges clinicians may face when selecting or being allocated to a role. While some teams, by virtue of pre-allocation or set professional roles may find less difficulty in role allocation, ad hoc and professionally homogenous teams may find this more demanding, leading to poorer performance [34]. Case 1 identified some team members unknowingly self-allocated into a role they were not suited. Poor self-assessment and conflicting perceptions of role responsibilities have been raised as a concern in emergency teams [35,36]; therefore, team members should have a clear understanding of role responsibilities and expected standards to enable effective role allocation.
The example of the scribe role in this study provides an excellent example of this point. To avoid poor levels of documentation in emergencies, senior staff should be allocated to the scribe role who can function in a secondary leadership role [37]. Throughout the study day debriefing discussions highlighted this point, and as the team members gained a greater understanding of the role responsibilities, midwifery students did not receive this role and a senior midwife was appointed to this role in Case 2. This finding suggests that future training courses should incorporate prerequisite knowledge of roles and role-related responsibilities, providing specific training (e.g. in scribing) to optimize team performance. Cross-training may be beneficial in order to ensure the roles with greatest clinical priority are attended to first with the additional benefit of improving shared mental models [38,39].
Despite participants views that leadership was important in enabling role allocation, both cases lacked explicitly allocated leaders. Role allocation was not verbalized by either the implied leader(s) or the team members themselves. While expert teams might prefer this style of implicit co-ordination, in high-stakes emergencies, more explicit co-ordination is recommended [32]. There was little discussion of the leadership role in the debriefings, or the lack of verbal allocation of leadership or roles, which is a concern given the importance of leadership team coordination and performance [40,41]. A possible reason for the lack of focus on leadership was in regards to instructors. Despite role allocation being discussed throughout the day, there was still evidence of maldistribution of workload in Case 2, which could potentially have been improved by clearer allocation of roles, via a leader. However, during the debriefing, while role allocation was raised by instructors, there was no specific feedback on the quality of role performance, such as a leader’s specific tasks. Objective feedback is important to learner development [42,43] and without such specific feedback, participants may have found it difficult to understand how to improve. A possible solution could be the development of a detailed model of competency [44] based on the role responsibilities outlined in Table 1, which could be used for formative assessment in simulation.
Although there remained some workload maldistribution in Case 2, the study subjectively demonstrated increased role consistency between Case 1 and Case 2 particularly in the role of scribe. Despite a lack of specific feedback regarding individual’s role-related performance, these improvements may still be related to team learning and reflection regarding use of the maternity team model throughout the day. The maternity team model introduced prior to Case 1, seemed to provide participants a focus for discussion regarding individual performance within the team and enabled reflections on how individuals might contribute most effectively through role allocation aligned with their individual skills and confidence levels. They describe the model as providing permission to ‘stay in role’ rather than constantly seek new tasks, which could be distracting or adding to a sense of chaos to the team environment. They expressed a decreased sense of guilt when doing ‘nothing’ and felt more in control when they could focus on the tasks within their role. Ongoing reassurance that periods of ‘inactivity’ in an individual’s role are a part of effective team function [45] may support team members transition to a pit crew approach. Furthermore, reframing these periods of ‘inactivity’ as opportunities for mutual performance monitoring may provide focus and further enhance team performance. This perceptual shift regarding role allocation, and the impact of individual performance on overall teamwork appeared to be mediated through the reflective discussions in debriefing, consistent with previous evidence highlighting the key role of debriefing in learning through simulation [46].
Using detailed video analysis provides insights into team performance which enrich the interpretation of the outcomes from the thematic analysis. Despite the richness of the data in this study, it represents only a small sample, and further research will be required to better understand the phenomenon of how clinicians learn and perform role allocation within maternity teams. Simulation does not always represent real life; however, it is an accepted modality in which to study human behaviour in settings where real-life research is not easily performed due to patient privacy or research feasibility concerns [47].
Conducting video analysis in detail is challenging and, in this study, multiple researchers conducted the analysis and discussed the results to achieve consensus. The process was time-consuming and required good-quality video from multiple angles and high-quality audio to observe the team interactions and behaviours.
The nature of this case study precludes forming any conclusions regarding the relationship between any system of role allocation and team performance; however, does provide a basis for further exploration of this topic within the maternity context. The researchers analysed the data through the lens of role allocation and their perceptions and beliefs with respect to role allocation may have influenced the analysis and interpretation of the data.
Effective role allocation in maternity emergencies appears to be contingent on participants firstly understanding the situation, knowing what needs to be done, and having suitable skills and confidence in role performance. Simulation training and debriefing may help participants alter their perceptions of effective role allocation and performance in roles. This study provides valuable insights to inform maternity emergency team training, namely the importance of providing learners with a detailed understanding of role responsibilities if they are to allocate team members effectively and perform well in these roles. Future research is required to determine how to best train, assess and provide feedback on team role allocation to improve team performance.
Supplementary data are available at The International Journal of Healthcare Simulation online.
None declared.
Dr Kikkawa was supported by a Griffith Institute for Educational Research seed grant in 2017.
None declared.
The ethics were approved by the relevant Human Research Ethical Committees (HREC/17/MHS/120; GUHREC/2018/560) and all participants provided written informed consent to participate in this study.
The authors declare they have no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
 How do maternity teams perform in and perceive a role-based approach to teamwork in maternity emergencies? A qualitative study in simulation
How do maternity teams perform in and perceive a role-based approach to teamwork in maternity emergencies? A qualitative study in simulation
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets