
There is a scarcity of simulation-based interprofessional (IP) programs in Portugal, with a notorious absence in undergraduate education. This paper describes the first step towards the development of an interprofessional education (IPE) undergraduate program, namely the implementation and preliminary assessment of the workshop LINKS – Lifting INterprofessional Knowledge through Simulation. The aim of this pilot study was to assess the educational effect of LINKS, in medical and nursing undergraduate students’ attitudes towards IP teamwork and collaborative practices, and their perception of roles and competencies within an IP team.
A total of 23 final-year students participated in the workshop. Teams of three or four elements (medical and nursing students) were exposed to two critical patient management simulation scenarios. To assess the impact of the workshop on students’ perception of IP collaborative practice, two surveys (ATTITUDES and IPEC) were applied before and after the workshop. Additionally, students’ opinion/satisfaction towards the workshop and its curricular integration was explored.
Students’ awareness of the relevancy of IP learning and self-competency in IP practice improved. For all subdomains and overall scores, statistically significant differences were found when comparing the pre- and post-scores, for both medical and nursing students, in both surveys. All students agreed that the workshop added educational value to their training, and recommended its integration in the formal curriculum, with a first round in the penultimate year and repeated in the last year.
Considering the pre–post test results and anecdotal comments shared during the session, we may infer that this single IPE event contributed to a clearer understanding of the team dynamic and individual role definition, increased the motivation to engage in collaborative practice between physicians and nurses and potentially challenged pre-existent stereotypes of each professional group. These findings corroborate the need for sustainable simulation-based IP programs, integrated in the undergraduate curricula, promoting early clinical interactions of different professional groups. We envision that the results of this study can help to inform future curriculum planning and provide useful insights that can be used within and between Portuguese institutions to develop a common IP undergraduate program.
What this study adds
The constant evolution and multiple challenges that healthcare systems face advocate for more team-based approaches [1]. Considering that many healthcare incidents are associated with team communication problems and deficient teamwork skills, effective collaboration and communication among healthcare team members are critical components for high-quality patient care [2]. Clinical errors can cause human suffering or even death and are, nonetheless, financially costly [3,4].
Physicians, nurses and other allied healthcare professionals work together on a daily basis at the postgraduate level. Despite this fact, most undergraduate curricula are separate and the training of effective communication strategies and care participation is often postponed to the future professional practice [5]. Traditional medical and nursing education is still based in professional silos, and students have expressed concerns on their insufficient understanding of other healthcare professionals’ roles and responsibilities, materializing the need for undergraduate interprofessional education (IPE) programs [6,7].
IPE is defined by the World Health Organization (WHO) as when ‘students from two or more professions learn about, from and with each other to enable effective collaboration and improve health outcomes’ [8]. Creating a culture that values teamwork and mutual space for students to learn with and from one another paves the way to success in preparing future healthcare professionals [9]. Studies show that IPE increases confidence in health professionals’ identity and appreciation of the roles of other professions, and improves communication, team-working skills [8,10,11] and quality of care [12].
Simulation-based training (SBT) is a well-accepted educational strategy that promotes the development of teamwork skills [13–15], being broadly used in current IPE programs that are slowly arising in medical and nursing schools [16]. This educational strategy can be effective in improving communication and collaboration among healthcare students [17], and its integration with IPE has been extensively recommended by WHO and several scientific societies to enhance IPE outcomes [10,18,19]. Several efforts have been made to create a framework towards a standardized undergraduate interprofessional (IP) intervention [11], including using SBT [20]. Nevertheless, the implementation and sustainability of these interventions are, many times, impaired by the stakeholders involved in the organizational change [21].
In the Portuguese healthcare educational context, simulation-based IPE programs for postgraduate education are emerging and, in specific contexts, have been successfully running for over a decade [22]. Opposed to that, undergraduate IPE in healthcare is barely existent. The Portuguese medical and nursing curricula make little to no reference to IP competencies and challenges and, if addressed, are limited to elective curricular units without a holistic integration in the curricula. Although, during their clinical rotations, students from different professions share the same clinical spaces and patients, no task blending or direct interaction between them occurs.
Considering the emergent educational need and the existent guiding frameworks [11,20,21,23], a collaboration between the Faculty of Medicine of University of Porto (FMUP) and Nursing School of Porto (ESEP), Portugal, was established, and a step-wise approach for the development of an integrative and sustainable IPE undergraduate program is currently being followed. This paper describes the first step towards this goal, namely the implementation and preliminary assessment of the program ‘Lifting INterprofessional Knowledge through Simulation (LINKS)’. LINKS is a simulation-based workshop targeting IP teams of healthcare students (medicine and nursing), aiming the development of IP team practices and behavioural skills to promote effective IP teamwork. To our best knowledge, this is a pioneer initiative that may contribute to a shift in the Portuguese healthcare education paradigm.
With this preliminary study we aim to assess the educational effect of this simulation-based workshop, in medical and nursing undergraduate students’ attitudes towards IP teamwork and collaborative practices, and their perception of roles and competencies within an IP team. A secondary objective is to explore students’ opinion towards the workshop and its curricular integration.
A pre–post design was used to explore changes in measures through the quantitative surveys completed by medical and nursing students that participated in the simulation-based IP workshop. A follow-up post-workshop questionnaire was used to assessed participants’ opinion. Detailed description of the data collection instruments is given below.
The outcome measurements fit in the first two levels of the extended version of Kirkpatrick’s classic educational outcomes model [24], with the quantitative surveys assessing modifications of attitudes/perceptions (L2A) and the post-workshop questionnaire assessing students’ reactions (L1).
Figure 1 presents a CONSORT flowchart for this single-arm, non-randomized, quasi-experimental study. Appendix 1 (Supplementary file) presents the extended CONSORT checklist for simulation-based research [25], for a comprehensive description of the present study.

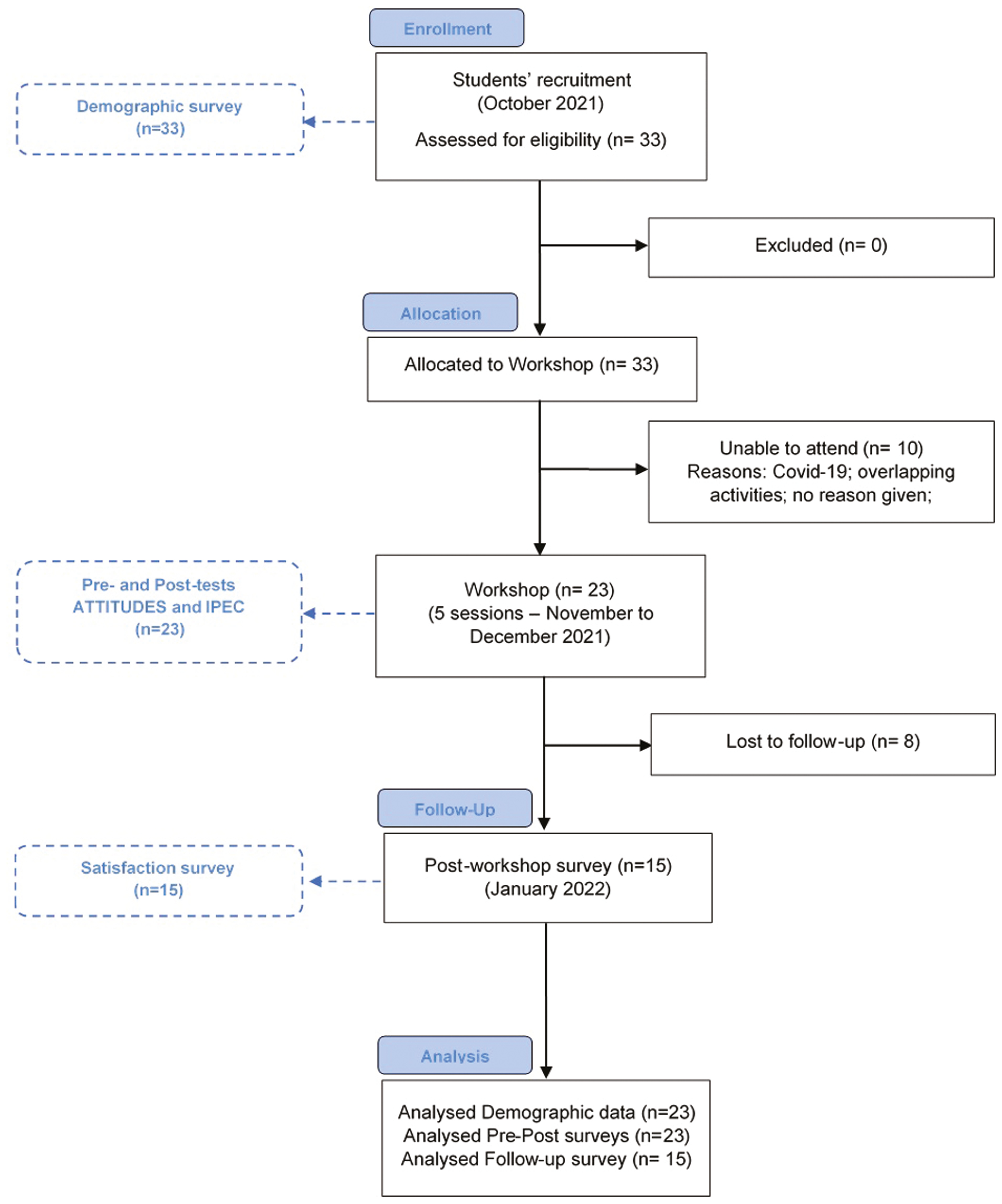
CONSORT flow diagram for a single-arm, non-randomized study of the workshop LINKS (Lifting INterprofessional Knowledge through Simulation).
All procedures followed general ethical standards and were in accordance with the principles outlined in the Declaration of Helsinki of 1975 (in its most recently amended version). This study was approved by the Ethical Committee of the Faculty of Medicine of University of Porto (31/CEFMUP/21). Written informed consent was obtained from all participants included in the study. All data were properly anonymized.
The recruitment of the participants was made by convenience sampling (non-probabilistic). All final-year students (287 sixth-year medical students and 42 fourth-year nursing students) were invited to participate in the workshop via e-mail.
Final-year students were selected considering that both medical and nursing students would have competencies and clinical skills for essential treatments, acquired in core clinical clerkships and have basic competencies for coping with emergency situations. Moreover, participants of this study are at the stage before starting their jobs and are capable to assess their competencies.
Vacancies were limited to eight students per session (four medical and four nursing), with a minimum of six students. At least, two students of each area (medicine/nursing) were needed to run a session. While enrolling the workshop, students were asked to select a date from those available and fill a simple demographic survey. Students were selected in a first-come-first-served basis. The recruitment was open for 2 weeks. After this period, participants received confirmation of their acceptance in the workshop with the information of the date, and were given basic information on ABCDE approach, cardiac arrest management and NTS, in an audio-visual support to promote students’ engagement and facilitate the review of relevant content.
All participants were informed of the voluntary nature of their participation, in advance. In each session, a group of 6–8 students was distributed in two IP teams. Teams of three or four elements were exposed to two critical patient management scenarios. All participants actively participated in both scenarios.
Each workshop was conducted between November and December, 2021, with a duration of 4 h, at the Clinical Simulation Centre of Faculty of Medicine of University of Porto. It started with an ice-breaking activity, involving all participants, followed by two clinical simulation scenarios, specifically designed for this workshop, aiming to challenge the clinical team to apply both technical and behavioural skills. Students were not informed of the scenario in advance, and assumed roles close to their professional competencies. In each scenario, the initial assessment was conducted either by nursing students (in the role of nurses) or by a team of one nursing and one medical student (assuming the roles of nurse and doctor). Typically, with patient deterioration, the initial team called the remain element(s) and began the management of the patient. Figure 2 illustrates a simulated scenario, during one of the sessions.
Illustrative image of a simulation scenario (multi-patient setting) during one session of the workshop.
The first scenario presented a patient with an anaphylactic shock followed by a cardiopulmonary arrest. This scenario explored the critical patient systematic approach and the application of resuscitation maneuvers in cardiopulmonary resuscitation context. It provided a context to reflect on how situational awareness evolved throughout the scenario, how leadership was established and how communication was developed in the various moments of the scenario.
The second scenario presented a multi-patient setting (two patients in a ward): one developing a post-op hypovolemic shock and the other requesting urgent pain control management. This provided a context to reflect on the importance of systematic assessment and re-evaluation, how the cooperation/interaction/support of team members has evolved, how the situational awareness changed throughout the scenario and how the communication of critical information (especially in a noisy environment) was established.
Each scenario took 15–20 min to unfold and was followed by a 40–50 min debriefing, conducted by a pair of experienced faculty members. The program details and approximated timings are summarized in Table 1.

| Component | Time | Content |
|---|---|---|
| Introduction (all) | 20 min | Introduction to the workshop and operational processes; introduction of the study and informed consent obtained; pre-test questionnaires filled |
| Ice-breaking activity (all) | 20 min | ‘Tangled’ is an interactive activity that allows the review of team dynamics and concepts |
| Briefing (all) | 15 min | Introduction of ground rules, overall learning objectives, confidentiality and psychological safety; familiarization with the simulation space and simulators |
| Simulation 1 (team of 3–4 elements) | 20–25 min | Scenario: anaphylactic shock with cardiopulmonary arrest |
| Debriefing 1 (team of 3–4 elements) | 40–50 min | Reflective discussion on team performance, based on learning objectives |
| Coffee break (all) | 15 min | |
| Simulation 2 (team of 3–4 elements) | 20–25 min | Scenario: multiple patients (hypovolemic shock + pain control management) |
| Debriefing 2 (team of 3–4 elements) | 40–50 min | Reflective discussion on team performance, based on learning objectives |
| Closing session (all) | 20 min | Take-home messages; post-test questionnaires filled |
A basic demographic questionnaire was distributed during recruitment, and included age, gender, background (nursing or medical), previous degree, previous simulation experience, previous participation in an IP educational context and the ability to read and understand English at a level that would allow to complete questionnaires in that language. The student’s proficiency in English was considered an inclusion criterion.
To assess the impact of the workshop on students’ attitudes towards IP teamwork and collaborative practices, two published surveys [26–28] were applied before and after the workshop, in their original version. The selection of these instruments was based on a literature search and considering their complementarity to assess the research question of this study. Both tools have been previously reported to have validation, in IP samples of students from the USA [26–28].
Attitude Towards Teamwork in Training Undergoing Designed Educational Simulation (ATTITUDES) [26] questionnaire was designed to measure students’ perceptions and attitudes towards IPE, teamwork and simulation as a learning modality. It consists of a 30-item scale organized into five subfactors: IPE relevance (7 items), simulation relevance (5 items), communication (8 items), situation awareness (4 items) and roles and responsibilities (6 items). Questions are scored in a 5-point scale from ‘strongly disagree’ (1 point) to ‘strongly agree’ (5 points). Total score is the sum of all item scores. A higher total score indicates a more positive students’ attitude towards IP learning through simulation-based IPE.
Interprofessional Education Collaborative (IPEC) Competency [27,28] was designed to assess competencies related to collaborative practice at the healthcare degree program level through individual student self-assessment. This tool is composed by two subfactors: IP interaction (8 items) and IP value (8 items). A 5-point scale ranging from ‘strongly disagree’ (1 point) to ‘strongly agree’ (5 points) is used to score each item. Total score is the sum of all item scores. The higher the total score, the more students perceived as competent in IP practice.
The questionnaires were completed before (pre-session) and after (post-session) the workshop for logistical reasons and to not interfere with the expected educational impact of the session.
To assess the opinion/satisfaction of the students towards the workshop an informal survey was sent, via e-mail, 4–6 weeks after the intervention. The questionnaire assessed three areas: (1) Organization (invitation and registration, didactics and timing); (2) Workshop content and structure (learning objectives, scenario, debriefing and supportive environment); (3) Workshop feedback and recommendations (positive features, needs improvement features and educational value). All questions were scored in a 5-point scale from ‘strongly disagree’ (1 point) to ‘strongly agree’ (5 points), with the exception of ‘positive features’ and ‘needs improvement features’ that were open, non-mandatory questions.
All questionnaires were anonymous. The association between demographic, pre-, post- and satisfaction questionnaires was made through the attribution of a unique code to each student.
Statistical analysis was conducted using IBM SPSS Statistics® software, version 27.0. Both descriptive and inferential analyses were performed. Considering the reduced sample size, non-parametric tests were used for inter- and intra-groups comparisons, considering a significance level of 5%.
Descriptive statistical analyses were conducted to identify the demographic distribution of participants in this study. Wilcoxon signed-rank test was used to compare the mean difference between the pre- and post-test results of each scale item within the two subgroups of the sample (medical and nursing students). Mann–Whitney U test was used to compare the mean differences between the two subgroups. Internal consistency of questionnaire scores was assessed through Cronbach’s alpha.
A total of 23 students participated in the workshop. The participants included 14 nursing students (60.9%) with mean age of 21.6 years and 9 medical students (39.1%) with mean age of 23.0 years. There was a clear predominance of the female population with a total of 19 female students (82.6%) and 4 males (17.4%), with the female population being 4.74 times higher. This is in line with the observed gender distribution in Portuguese medical and nursing schools and in health systems in general [29]. Among the participants, 21 (91.3%) reported having previous simulation experience. Of all the participants, only four (17.4%) had previous IPE experience throughout their academic training. All students indicated to be proficient in English (capable to read and understand). The relevant demographic characteristics of the participants are summarized in Table 2.
| Medical (n = 9) | Nursing (n = 14) | |
|---|---|---|
| Mean age (years) | 23,0 | 21,6 |
| Gender (n) | ||
| Female | 7 | 12 |
| Male | 2 | 2 |
| Previous simulation experience (n) | ||
| Yes | 9 | 12 |
| No | 0 | 2 |
| Previous IPE experience (n) | ||
| Yes | 0 | 4 |
| No | 9 | 10 |
ATTITUDES and IPEC Competency scores for medical and nursing students before and after participating in IPE programs are shown in Table 3.
| Medical (n = 9) | Nursing (n = 14) | |||||
|---|---|---|---|---|---|---|
| M (SD) | P-value | M (SD) | P-value | |||
| ATTITUDES [26] (1 to 5 scale) | Relevance of IPE | Pre | 4.67 (0.27) | 0.018 | 4.66 (0.24) | 0.001 |
| Post | 4.97 (0.06) | 4.94 (0.12) | ||||
| Relevance of Simulation | Pre | 4.82 (0.19) | 0.038 | 4.66 (0.33) | 0.007 | |
| Post | 5.00 (0.00) | 4.89 (0.19) | ||||
| Communication | Pre | 4.70 (0.31) | 0.027 | 4.62 (0.29) | 0.010 | |
| Post | 4.96 (0.06) | 4.89 (0.21) | ||||
| Situation awareness | Pre | 4.56 (0.41) | 0.026 | 4.44 (0.41) | 0.027 | |
| Post | 4.92 (0.18) | 4.84 (0.30) | ||||
| Roles and responsibility | Pre | 4.48 (0.52) | 0.027 | 4.61 (0.32) | 0.027 | |
| Post | 4.96 (0.07) | 4.86 (0.26) | ||||
| Total | Pre | 4.65 (0.28) | 0.012 | 4.61 (0.21) | 0.002 | |
| Post | 4.96 (0.05) | 4.89 (0.16) | ||||
| IPEC Competency [27,28] (1 to 5 scale) | IP interaction | Pre | 3.35 (0.51) | 0.007 | 3.89 (0.66) | 0.003 |
| Post | 4.40 (0.56) | 4.64 (0.33) | ||||
| IP value* | Pre | 4.01 (0.44) | 0.011 | 4.54 (0.33) | 0.010 | |
| Post | 4.61 (0.43) | 4.87 (0.22) | ||||
| Total* | Pre | 3.68 (0.44) | 0.008 | 4.22 (0.45) | 0.003 | |
| Post | 4.51 (0.48) | 4.75 (0.24) |
Scores presented as mean (SD). Pre–post-test differences, Wilcoxon signed-rank test (α = 0.05). Statistically significant results presented in bold. Difference between groups, Mann–Whitney U test (α = 0.05). Intergroup differences were found in the pre-test scores marked with *.
Wilcoxon test was used to analyse the intragroup mean difference between the pre- and post-test results. The overall and subfactors ATTITUDES and IPEC Competency scores increased significantly after IPE, for both medical and nursing students.
Mann–Whitney test was used to analyse intergroup differences, both in pre-test and post-test scores. The only statistically significant difference found was in the pre-test scores of the ‘IP value’ (IPEC questionnaire), with concomitant difference in the pre-test IPEC overall score.
Internal consistency of measures was good (Cronbach 0.8 ≤ α < 0.9) for ATTITUDES scores and excellent (Cronbach α ≥ 0.9) for IPEC scores, showing that both scales present a high reliability for this sample. Table 4 presents the internal consistency values for each scale, for both pre- and post-test.
| Pre-test | Post-test | |
|---|---|---|
| ATTITUDES | 0.856 | 0.881 |
| IPEC Competency | 0.905 | 0.919 |
The follow-up opinion/satisfaction questionnaire had a total of 15 replies, with eight drop-outs. Overall, students agreed or completely agreed that the workshop was well-organized, with a clear and appropriate invitation, adequate bibliography sent in an attractive format (audio-visual) and adequate timing (mean: 4.60; SD: 0.37). All students agreed that this experience should be repeated within few months with different scenarios, and all but two agreed that the final year was the best timing for the workshop.
Similarly, the workshop content was rated high (mean: 4.83; SD: 0.23), with all but one agreeing that the learning objectives were clear, important and adequate (mean: 4.73; SD: 0.26), all agreeing that the scenarios were realistic, with adequate number and time (mean: 4.82; SD: 0.21), all agreeing that debriefing had a constructive approach, allowed reflection on individual and teamwork performance and was open to all contributions (mean: 4.93; SD: 0.14) and all but one agreeing that environment was supportive with psychological safety guaranteed (mean: 4.84; SD: 0.54).
All students agreed (mean: 5.00; SD: 0.00) that the workshop added educational value to their training, and recommended its integration in the formal curriculum (mean: 4.80; SD: 0.41), with a first round in the penultimate year and repeated in the last year. The open questions on ‘positive features’ and ‘needs improvement features’ were aligned with the previous opinions. The positive comments focused mostly in the IP interaction that the workshop offered (eight comments) with a few comments about the importance of debriefing (three comments) and the realism of scenarios (two comments). Possible improvements suggested by students were increasing time and frequency of the workshop (three comments), and provide additional didactics before the workshop (one comment).
The present study explored the educational effect of a simulation-based IP workshop (LINKS), in medical and nursing students’ attitudes towards IP teamwork and collaborative practices, and their perception of roles and competencies. This study found that both medical and nursing students increased their awareness on IP practice and changed their perception of roles and competencies within an IP healthcare team. These findings are in line with the results of the studies presented in the scoping review conducted by Langton et al. [16].
ATTITUDES and IPEC Competency scores showed, for both groups and for all subfactors, a statistically significant increase between the pre- and post-test, indicating a more positive attitude towards collaborative practice. Of notice is the IPEC Competency scores prominent increase in the ‘IP interaction’ subfactor, for both students’ group. These results reinforce that ‘working’ together can enhance the individual role and responsibility within the team, and predispose to further interactions.
The analysis of the intergroup differences for ATTITUDES subfactors indicate that, overall, both nursing and medical students had similar perspectives towards IPE, simulation, communication, situational awareness and their roles and responsibilities, at the baseline (pre-intervention) and after the workshop (post-intervention). Medical students’ IPEC mean scores at baseline, for both dimensions, were approximately half-point lower in comparison to nursing students mean scores, with statistically significant differences found in the ‘IP value’ (and, concomitantly, in the overall score). One possible explanation for this result may be that internships of nursing students are, in nature, more team-based than medical students’ internships. Nursing students are involved in various tasks, stimulating their integration within the team (which includes colleagues, tutors, doctors and auxiliary personal) and even with the patient and their families. On the other hand, medical students tend to be focused in technical tasks and engage only in specific activities attributed and oriented by the tutor. Notably, these differences in the baseline become flattened after the intervention, with medical and nursing students presenting higher scores and in the same range, an indicative of reciprocal IP attitudes.
Prior to this study, only four nursing students had IPE experience, even though both groups were in their final year of undergraduate studies and had already started clinical clerkships. The lack of exposure to clinical situations, that require collaboration with other professional groups, can affect students’ perceptions of IP collaboration and practice, and reinforce stereotypes that are prejudicial to effective teamwork.
The behavioural skills imbedded in the scenarios were used to foster open communication, shared information and decision-making, and mutual respect and trust. During debriefings, students reported to have gained: (1) a better understanding of the role of the other healthcare professionals, (2) a more positive attitude towards IP teamwork and (3) confidence in their teamwork skills. Reported examples highlighted the importance of structured communication (e.g. iSBAR – identification, situation, background, assessment and request/recommendation), which allowed the nursing students to share their concerns and provide regular and accurate patient information, and the benefits of summarizations, which stimulated medical students to share information and develop, within the team, a collaborative clinical reasoning and shared mental model.
Considering the pre–post test results and anecdotal comments shared during the session, we may infer that this single IPE event contributed to a clearer understanding of the team dynamic and individual role definition, increased the motivation to engage in collaborative practice between physicians and nurses and potentially challenged pre-existent stereotypes of each professional group. These results are consistent with other studies [30–36].
The majority of the students in this study had previous experience with SBT (with the exception of two nursing students). These findings demonstrate that simulation is a well-accepted educational strategy, commonly integrated in both nursing and medical curricula. On the other hand, the same level of importance and acceptance is not observed towards IPE, marked by separate academic pathways, despite the physical proximity that some nursing and medical schools have. The results of the follow-up satisfaction questionnaire corroborate these findings. It highlighted that students understand the importance of this educational approach, requesting for more opportunities to train and practice their IP skills, especially at the end stage of the undergraduate education. Although there were eight drop-outs, this feedback is a starting point to refine the workshop and understand what should be maintained and what should be improved in future interventions.
IP teamwork training in an educational controlled setting (such as in simulation-based activities) nurtures collaborative practices and develops a clear understanding of the role and contribution of the ‘other’. The educational benefit is observed even in single, short-term IP simulation activities, such as LINKS.
We envision that the results of this study can help to inform future curriculum planning and provide useful insights that can be used within and between institutions to develop a common IP undergraduate program.
The major limitation of this study lies in its reduced sample. The simulation centre and faculty availability, the limited number of people per room in confined spaces due to COVID-19 pandemic, and students’ overlapping clinical activities were the main barriers. A multi-centric study with a larger sample would be beneficial to provide external and ecological validities to the present study. Moreover, using a convenience sample (as opposed to a probabilistic sample) might lead to biased results due to the implicit predisposition to engage in an activity.
Although all participants had been enrolled in several clinical clerkships before the study, COVID-19 pandemic peak was during their undergraduate clinical years, which considerable limited their clinical experience and direct involvement with other healthcare professionals [37].
The outcome measurements of this study were based on self-reported, subjective assessment, which per se have an intrinsic bias [16]. Being a single event can also be considered a limiting factor, as different results may emerge after a regular and more consistent IPE program.
Regular IPE activities and respective data analysis could provide a deeper understanding of IPE long-term effects. A longitudinal study, with repeated measurements overtime would explore if there is long-lasting effect of IPE, and the need for a periodical IPE program.
Most healthcare educational system focusses mainly on a single-profession scientific learning, with major gaps in collaborative and teamwork-related skills. IPE undergraduate programs can reduce these gaps, promoting a better understanding of teamwork, roles and responsibilities within a team and professional identity. This study presents a pilot approach to this modality in Portugal and identifies the positive effects of simulation-based IPEs, highlighting meaningful information that could guide to future interventions and curricula revisions.
The study findings reinforce that IP interactions in an educational setting are well-received, perceived as relevant and can contribute to demystify students’ preconceived notions or stereotypes of other professions, particularly the hierarchy of decision-making between doctors and nurses.
While a single simulation-based IP session has educational benefits, more sustained opportunities could lead to greater advantages. Including simulation-based IP programs within the clinical practice would expose and challenge undergraduate students, on a regular basis, to actively interact with other professional groups. Although challenging to current healthcare educational programs, such initiatives are needed to foster content and process changes in the healthcare professionals’ curricula, so that these skills are perceived as core elements of good practice and higher quality of care.
Supplementary data are available at The International Journal of Healthcare Simulation online.
The authors would like to thank the students for their voluntary participation in the workshop and study.
All authors have made substantial contributions to the manuscript, namely: CS-C, FF, CCP, EL and CC contributed to the conception and design of the study; CS-C, FF, CCP, EL and CC implemented the study and collected the data; CS-C and FF analysed and interpreted the data; CS-C and FF drafted the article. CCP, EL and CC reviewed it critically for important intellectual content; all authors have approved the manuscript version submitted and agree with its submission.
This article was supported by National Funds through FCT - Fundação para a Ciência e a Tecnologia within CINTESIS, R&D Unit (reference UID/IC/4255/2019).
Data and materials are available upon reasonable request to the corresponding author (Carla Sá Couto, lead researcher).
The authors declare that all procedures followed general ethical standards and were in accordance with the principles outlined in the Declaration of Helsinki of 1975 (in its most recently amended version). This study was approved by the Ethical Committee of the Faculty of Medicine of University of Porto (31/CEFMUP/21). All data were properly anonymized. Written informed consent was obtained from all participants included in the study.
The authors declare no conflict of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
 Impact of a simulation-based interprofessional workshop (LINKS) on Portuguese healthcare students’ perception of roles and competencies: a quasi-experimental pilot study
Impact of a simulation-based interprofessional workshop (LINKS) on Portuguese healthcare students’ perception of roles and competencies: a quasi-experimental pilot study
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets