Corresponding author: Victor Cheung, [email protected]
” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-victorcheung”>Victor Cheung, 1 Multi-Disciplinary Simulation and Skills Centre, Queen Elizabeth Hospital, Kowloon, Hong Kong” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-eric-hang-kwongso”>Eric Hang-Kwong So, 2 Department of Surgery, University of Melbourne, Melbourne, Victoria, Australia” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-debranestel”>Debra Nestel, 1 Multi-Disciplinary Simulation and Skills Centre, Queen Elizabeth Hospital, Kowloon, Hong Kong” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-jeff-leung-kithung”>Jeff Leung-Kit Hung, 1 Multi-Disciplinary Simulation and Skills Centre, Queen Elizabeth Hospital, Kowloon, Hong Kong” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-sze-szeso”>Sze-Sze So, 1 Multi-Disciplinary Simulation and Skills Centre, Queen Elizabeth Hospital, Kowloon, Hong Kong” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-nam-hungchia”>Nam-Hung Chia, 1 Multi-Disciplinary Simulation and Skills Centre, Queen Elizabeth Hospital, Kowloon, Hong Kong” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-george-wing-yiung”>George Wing-Yiu Ng
With the advancement of innovative technology, healthcare professionals stand to benefit from adjustments to procedural skills training/assessment introduced during the COVID-19 pandemic. In this essay, we reflect on the development of a virtual reality (VR)-based training programme to support medical and nursing staff in procedural skills for central venous catheter (CVC) insertion, related communication skills and situation awareness. The remote delivery was a direct response to the impact of the pandemic and is likely to remain as an educational strategy on our centre.
What this study adds
The COVID-19 pandemic has changed the way many people work and live, and increased attention to a global trend of digitalization, including the impacts of remote work and education on staff well-being, organizational performance, and training effectiveness. Virtual reality (VR) has been shortlisted by a group of world-renowned healthcare leaders as one of the top 10 healthcare innovations alongside other cutting-edge technologies such as 3D-printed devices, artificial intelligence and telehealth [1].
VR has been used by clinical psychologists to work with patients suffering from anxiety attacks, psychosis, symptoms of Alzheimer’s disease, and acute or chronic pain or disability in a variety of settings including rehabilitation wards, outpatient units and community settings [2–5]. For example, immersive experiences where clients are exposed to specific stressors (e.g. crowed scene, dirty environment, spiders) could help them to progressively cope with that undesirable stimulus in a controlled environment [2]. Beyond clinical applications, VR has another potential use in supporting training and development of healthcare professionals [6].
In a meta-analysis of 92 studies examining technical and socio-emotional skills development using VR, Angel-Urdinola and colleagues highlighted that 78% of studies found comparable or better learning outcomes than traditional classroom teaching, including greater increases in confidence, self-efficacy, and efficiency as well as lower error rates (e.g. emergency evacuation of neonates, procedural sedation, robotic suturing, etc.) in diverse health and surgical education contexts [7]. Blumstein and colleagues conducted a randomized controlled trial (RCT) of training for surgical management of tibial shaft fractures, in which they randomly assigned 20 medical students into an experimental group with VR as a major training modality or a control group with a learning guide [8]. Medical students in the experimental group had assessment scores that were 2.3 times higher than their counterparts in the control group, as well as demonstrating greater accuracy and reduced procedure times [8]. In this essay, we share our experience in developing a VR-based training for healthcare professionals after a brief summary of related background information and research findings.
Central venous catheter (CVC) insertion is a medical procedure during which a doctor, with the assistance of a nurse or other health professional, places a catheter into a large vein, such as the internal jugular vein at the neck, subclavian and/or axillary vein on the chest, or femoral vein at around the groin [9–11]. This procedure is commonly used in clinical departments for haemodialysis (i.e. the administration of fluids and medications where using a peripheral vein is no longer available) and for hemodynamic monitoring [11–13]. CVC can lead to lethal complications following clinician errors such as failure to remove the guidewire, including but not limited to arrhythmias, myocardial perforation, central line-associated bloodstream infections (CLABSIs) and thrombosis [8,10,12,14]. Therefore, there is a need to ensure that clinicians are provided with highly effective training that reduces error rates as much as possible [7].
Formal training is necessary to ensure a quality service and protect patient safety. Traditional training on real patients whilst guided by an experienced supervisor may still be prone to patient safety issues. Beyond simply understanding anatomical landmarks, surgical trainees require hands-on practice in a variety of surgical procedures to enhance cognitive knowledge of procedural steps and related surgical skills associated with tactile sensation [11,14]. Practice on real patients in a mentorship programme with experienced surgeons at consultant levels may result in experiences gained at high costs, in terms of higher risk ratio of mortality or complication (10%–25%), lack of opportunity for training in critical but rare procedures, inflexibility in training schedules and suboptimal use of clinical supervisor time [10,11]. VR enables healthcare professionals to practise the steps of certain clinical procedures in a virtual setting, prior to performing the same procedures on real patients [6]. It can avoid unethical practice (e.g. violating general principles of beneficence/non-maleficence and competence in service provision) and can also ensure the quality and safety of healthcare services to safeguard the best interests of both service providers and users. An advanced training modality, such as part-task trainer (a device for training in CVC procedures in this study), is an alternative for the ‘see one, do one, teach one’ training model on real patients [10,14].
Despite scientifically proven enhancements in procedural skills, cognitive and affective aspects (including communication skills and empathy) cannot be addressed as easily through practice on part-task trainers [14]. Guetterman and colleagues used VR to examine how medical students reacted to a simulated patient when breaking bad news (e.g. end-of-life issues for decision of do-not-resuscitate, DNR) during scenario-based simulation training [15]. The results were encouraging; with the support of VR technology, their research team found that medical students would be able to share bad news with the patient or relative in a caring manner [15]. Another study by Dyer and colleagues supported their findings, adding that medical students’ professionalism was improved, particularly with elderly patients [16].
The Multi-Disciplinary Simulation & Skills Centre (MDSSC), a hospital-based simulation training centre in Queen Elizabeth Hospital (Hong Kong) has been changing healthcare education in alignment with organizational needs and international education, assessment and research standards. In order to develop an effective healthcare education programme, our multidisciplinary team started with needs identification, linking training objectives to results based on root cause analysis, a thorough investigation on leading cause of medical incidents (see Table 1 for composition of multidisciplinary team and related KSAOs).

| Role | Knowledge, Skills, Abilities, Other factors (KSAOs) |
|---|---|
| Centre Directors/ Training Advisors | – who are specialized in surgery, anaesthesiology or intensive care at consultant level – skilful in performing central venous catheter (CVC) insertion procedures on real patients with experience in teaching CVC – able to apply extensive experience in clinical practice, knowledge and skills to develop simulation-based training with elements in crew resources management for patient safety climate – able to provide professional advice on standard procedures of CVC, setting of the simulation environment, with visionary mind-set |
| Centre Manager/ Administrator | – who are knowledgeable in procurement policy and operational guideline. – skilful in project and cost management, showing ability to build teams with good work ethics as well as systematic workflow under healthy and safety culture. – able to monitor system process with prior training in leadership skills, and communicate effectively with stakeholders at all levels |
| Research Officer | – who holds post-graduate qualification in occupational psychology with professional qualification as Registered Psychologist and Certified Healthcare Simulation Educator (CHSE) of Society of Simulation in Healthcare (SSH) – skilful in conducting scientific research project planning and management, data analysis, and psychometric assessment – able to perform abstract thinking, reasoning and problem solving; willing to work independently with adventurous and creative mind-set |
| Technician/Programmer | – who are at their sophomore or junior year in computer science or engineering major with professional experience in VR programme design – skilful in graphic design and practicable knowledge in VR software (e.g. Unity) – able to inform decision in model prototyping, with curiosity and motivation for innovation as a team player |
| Simulation Operations Specialist | – who are knowledgeable in chemistry with professional qualification in Certified Healthcare Simulation Operation Specialist (CHSOS) of Society of Simulation in Healthcare (SSH) – skilful in simulation environment preparation and set-up for training with VR programme – able to give advice on feasibility training modality as well as tentative flow, with innovative mind-set as a team player |
| Executive Assistant | -who plays active role at supporting rank in providing administrative, operational and technical support throughout the training process -able to provide clear instruction to instructors and participants in preparation phase, and maintain training and evaluation record according to service guideline and advice from program director and coordinator |
In 2017, a hospital annual report on sentinel and serious untoward events regarding five CVC-related medical incidents raised public awareness of guidewire retentions following CVC insertion procedures, including the irreversible harm caused to patients, the negative impacts on self-efficacy of involved staff and damages to community trust [17]. In 2021, the Quality & Safety Department of Hospital Authority Head Office highlighted several recommendations at ‘Hospital Authority Risk Alert’ for the service enhancement plan [18]:
ii) To improve communication to healthcare professionals regarding clear role delineation and responsibilities.
ii) To strengthen knowledge and skills among doctors and nurses by organizing training in CVC procedures and after care, and reinforcing ‘1-set-1-time’ practice.
iii) To strictly monitor compliance to CVC insertion guidelines, reinforce critical checking steps between doctors and nurses, and update bedside procedure safety checklist with standard workflow.
We developed a tailored VR programme to train doctors and nurses in CVC procedures in line the service enhancement plan. Distinctive from simulation training of CVC with a part-task trainer, our tailored VR programme synchronizes two sets of devices, enabling one doctor and one nurse to engage simultaneously in the entire CVC insertion procedure (see Table 2).
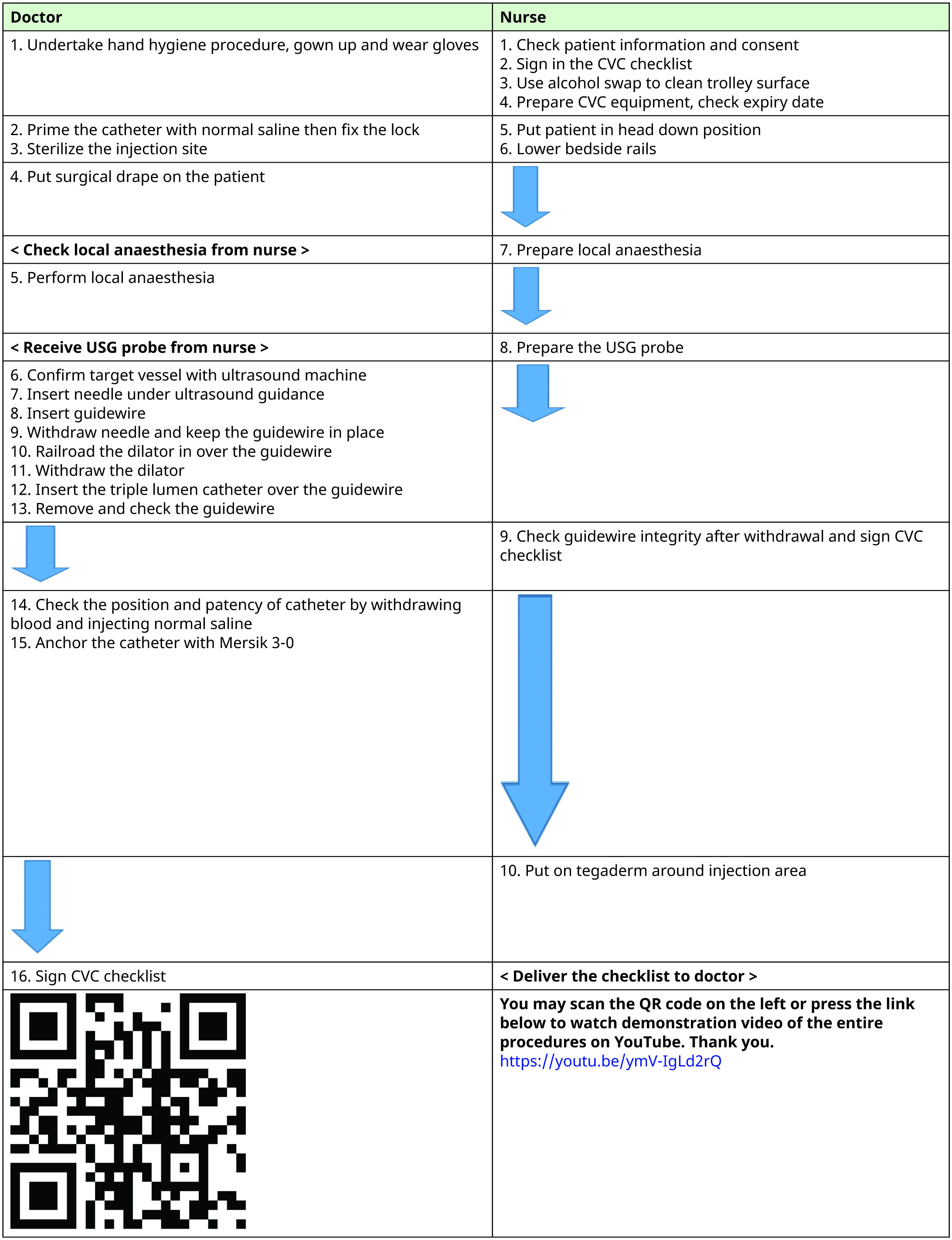
This feature strengthens teamwork and communication skills between doctors and nurses during the procedure, as well as their situation awareness (e.g. knowing when to prepare the ultrasound probe, pass equipment to the doctor, remind the doctor of missing a step with checklist) through interacting with the other professional’s ‘avatar’ within the virtual learning environment. This training modality is compatible with tele-education, enabling participants to attend the training at any site with equipment required, such as host computer, base station and head-mounted display. The space of the room for VR should be not less than 6.6 square feet (see Figure 1).

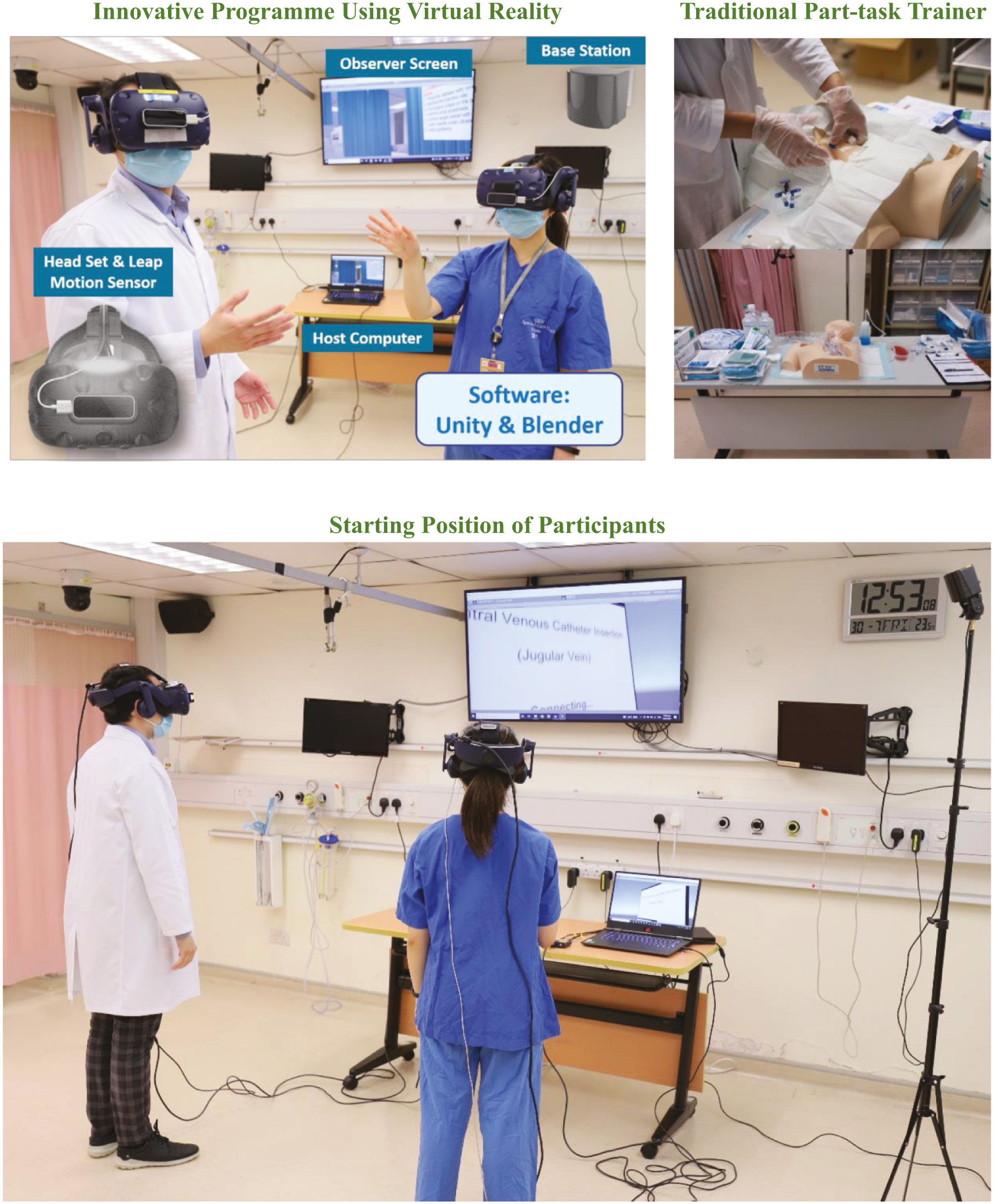
Equipment/setting of virtual reality programme and traditional part-task trainer.
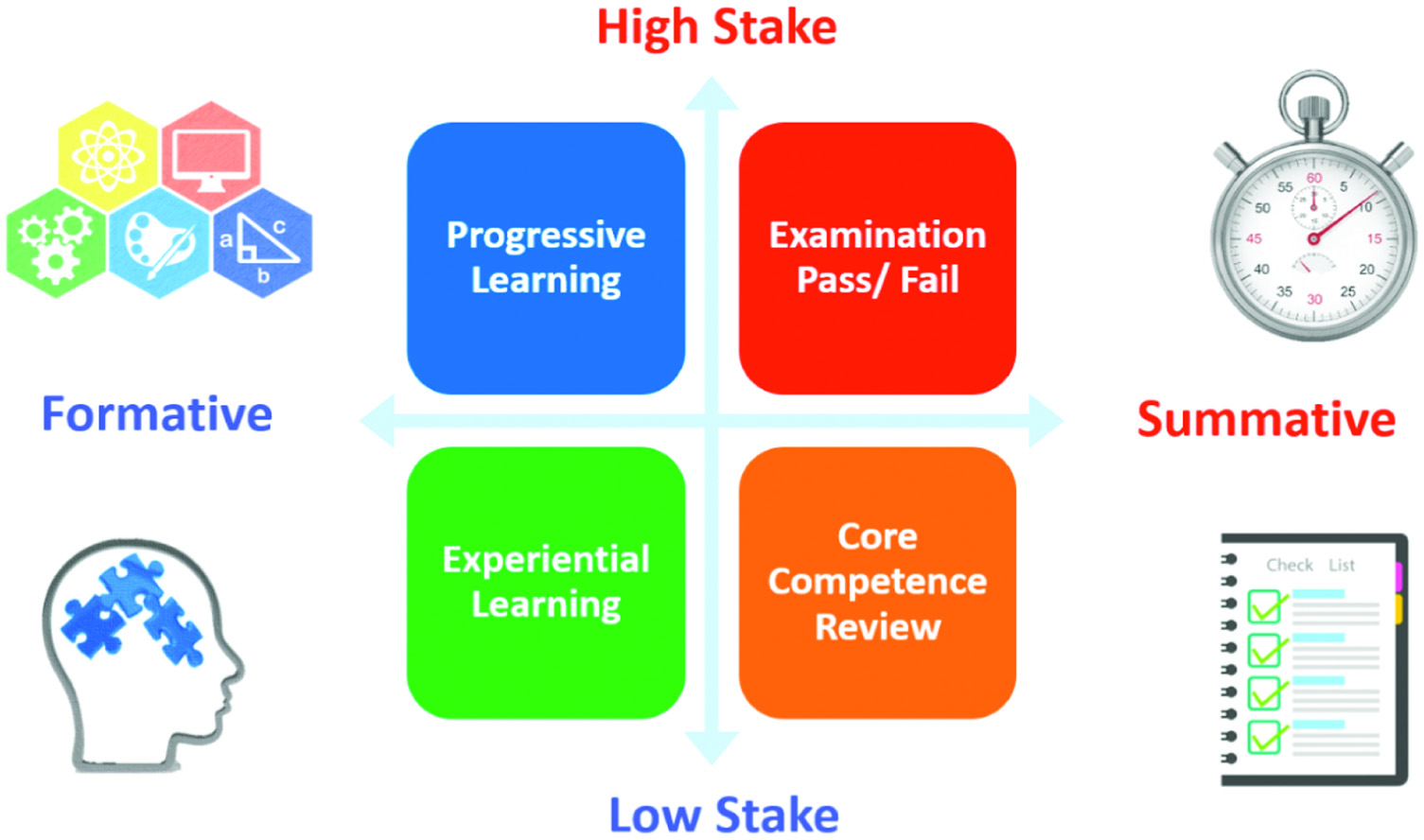
Quadrant chart of training/assessment type and level.
This is the first locally developed multi-purpose VR-based programme for CVC training in our lab-based simulation centre. To maximize learning effectiveness, the programme has been planned to be incorporated into existing CVC insertion training for medical and nursing staff in the Queen Elizabeth Hospital. In a sense of innovation that creates system-wide synergies, procedural knowledge can be diffused to inter-hospital service, and from simulation training to day-to-day clinical practice. The programme demonstrates its strengths on flexibility and versatility, enabling educators to assess performance of participants in variety of types (formative or summative) and levels (low or high stakes) in four quadrants (see Figure 2).
For example, compliance rate with standardized checklists or time to complete the task can be evaluated as one of the measurable outcomes for quantification of the skills participants gain at the end of the training for low-stakes summative purpose. Prior to full implementation of the VR programme for post-graduate staff, dry-run sessions were made to elicit user feedback for final adjustment on graphic design, overall arrangement and logistics of the training, and preliminary evaluation on training satisfaction, as well as their acceptance of VR as a standalone training modality for CVC insertion procedures.
As well as effectiveness, the acceptability and practicability of any training programme play a major role in achieving training objectives. According to our preliminary feedback from dry-run sessions, using VR as a training modality has been widely accepted by major stakeholders for several reasons. As opposed to traditional classroom teaching and hands-on practice, participants found themselves highly motivated to learn with high technology, interactive element, as well as a simple but smart interface [6]. Through immersive experiences with the VR programme, participants would not only be able to acquire procedural skills of CVC insertion but also enhance communication skills as well as situation awareness of near-miss between doctor and nurse pairs transferable to daily clinical operations. The VR-based training relies on fewer human resources because it is operated by a pair of participants plus or minus on-site or distanced technical supports. Beyond learning effects right after the training session, long-term benefits reflected by change in human resources in balance of monetary investment on VR programme development and patient safety could be expected (e.g. reduced length of stay, costs on additional medical expenses or even litigation due to post-CVC complications). Such potential impacts probably explain why hospital management worldwide showed higher acceptance of incorporating high technology into regular training programme for healthcare professionals amid the COVID-19 pandemic.
Further research could explore service effectiveness of incorporating CVC VR programme into formal simulation training curriculum at 6 dimensions bounded by the modified Kirkpatrick’s model [19], which includes:
– Level 0 – Activity Accounting (Curriculum, Training Objectives, Success of Organization Change)
– Level 1 – Reaction (User Satisfaction)
– Level 2 – Learning (Acquisition of Knowledge and Skills)
– Level 3 – Behaviour (Personal Strengths/Knowledge and Skills Transfer)
– Level 4 – Results (Clinical Performance/Organizational Impacts)
– Level 5 – Return on Investment or Expectation (ROI/ROE, including Monetary and Societal Impacts)
Examining these measurable outcomes may help us reinforce evidence-based practice in the way that healthcare management systems are well connected with task-specific training, assessment and innovative research [19–22].
We would like to express our gratitude to Kowloon Central Cluster hospital management for on-going support to simulation training development and administrative and technical staff members of the Multi-Disciplinary Simulation and Skills Centre for intellectual input in converting creative ideas into actionable training program.
All authors contributed to the concept or design, acquisition of data, and analysis or interpretation of data. All authors critically reviewed and revised the draft from the first author for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
None declared.
None declared.
None declared.
None declared.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
 Exploring the content validity of Clinical Cultural Competence Questionnaire in diverse cultures
Exploring the content validity of Clinical Cultural Competence Questionnaire in diverse cultures
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets