
Introduction Increasingly more resources are being used internationally in training and educating qualified healthcare personnel due to high personnel flow and rapid development within technology, care and treatment. Consequently, transferring learning from simulation-based training to competency in clinical practice is an essential question for healthcare faculty and management. Nevertheless, there is no established method for assessing if transfer occurs. This article aims to demonstrate how a hybrid method can explore transfer of learning from a simulation-based course to competency in clinical practice. Methods The hybrid method consists of a phenomenological–hermeneutic Ricœur-inspired analytical approach and a Cognitive Event Analysis of ethnographic data from a healthcare setting. Discussion It is argued that this hybrid method can gain awareness of behavioural changes following a simulation-based training course and how transfer happens. It is concluded that the hybrid method can provide insights into complex actions and constitutes a systematic and detailed approach to capturing transfer of human factor skills from simulation-based training to competency in critical practice. This research is the first step in developing a tool of transfer.
What this study adds
Internationally, simulation-based training (SBT) is increasingly used in healthcare to train qualified personnel’s technical and human factor skills1 (HFS) [1]. Consequently, there is a need to understand if and how HFS transfers from SBT to competency2 [2] in everyday clinical practice.
This article argues that a hybrid method is needed to clarify how knowledge and competencies are transferred from SBT into competency in clinical practice. Due to the complexity of tracking changes inb human behaviour, such a hybrid method must comprise at least (1) a theoretical framework that integrates social, psychological and cognitive aspects of behaviour; (2) methods for describing, understanding and explaining how HFS can become clinical competency; and (3) a factual investigation into how HFS is taught and adapted into complex clinical practice. This article proposes that combining a broad theoretical framework and hybridity of methods can provide insights into the effectiveness of SBT in improving healthcare personnel’s HFS performance in clinical practice.
A new way of analysing ethnographic data from a Danish healthcare setting is presented with a hybrid of both a phenomenological–hermeneutic approach of being in the world (Ricœur) [3] and a cognitive ethnographic approach to track the conception and execution of tasks in cognitive systems (Hutchins) [4]. A hybrid method that can gain insight into how transfer of learning occurs in practice through specific descriptions of cognitive events and validated interpretations of similar events.
A recent systematic review [5] reveals that methods for assessing HFS in healthcare SBT are varied and inadequate and that HFS is often trained in interaction with technical skills training. Abildgren et al. show that when HFS is taught simultaneously with technical skills, HFS often becomes a secondary focus to medical knowledge (e.g. diagnosis, procedures and treatment), and technical skills become preferred learning objectives. Furthermore, when SBT courses emphasise HFS, it is often done through reductive checklists and acronyms (e.g. A–E principles, SBAR), and HFS is often codified as technical-related skills (e.g. behaviour markers: asking for timeout, taking the leadership, delegating tasks ) to make them visible for monitoring. The conflation of technical skills with HFS adds further challenges to assessing transfer [5].
Research on SBT has established that technical skills improve professional performance and bring novices to a higher performance level sooner than if they had to learn the same skill through apprenticeship [6–8]. However, it needs to be determined if SBT of HFS is beneficial to the same degree. The lack of knowledge on HFS training is potentially due to the absence of concrete methods for monitoring transfer of HFS after SBT or the difference between HFS and technical skills. Monitoring potential improvements in HFS is more complex than monitoring technical skills. Furthermore, cognitive, social, interactive and situational factors are often not interactionally visible nor easily quantifiable. Therefore, reporting on these elements demands a divided awareness and aligned perception of the HFS within the assessors [9,10].
Researchers [11–15] have explored HFS by assessing behaviour and behaviour changes among healthcare personnel using observational studies combined with different assessment methods. These studies typically focus on the performance progress within the simulation scenarios, immediately before and after SBT, assessed by pre-and post-tests (knowledge), pre-and post-scenario (following algorithms or acronyms), behaviour makers or numbers of adverse events (patient safety). The weakness of such approaches is the need to track how HFS training transfers to competency in daily practice. Similarly, research establishes that adding knowledge only sometimes leads to new competency in everyday practice [16,17]. Knowing is not the same as performing. Humans are living organisms comprehending as they act and vice versa [18]. Consequently, to provide evidence of the effectiveness of SBT in improving HFS, there is a need for a method that describes, understands and explains how transfer of HFS from SBT to competency happens. The existing methods are either limited to describing or explaining.
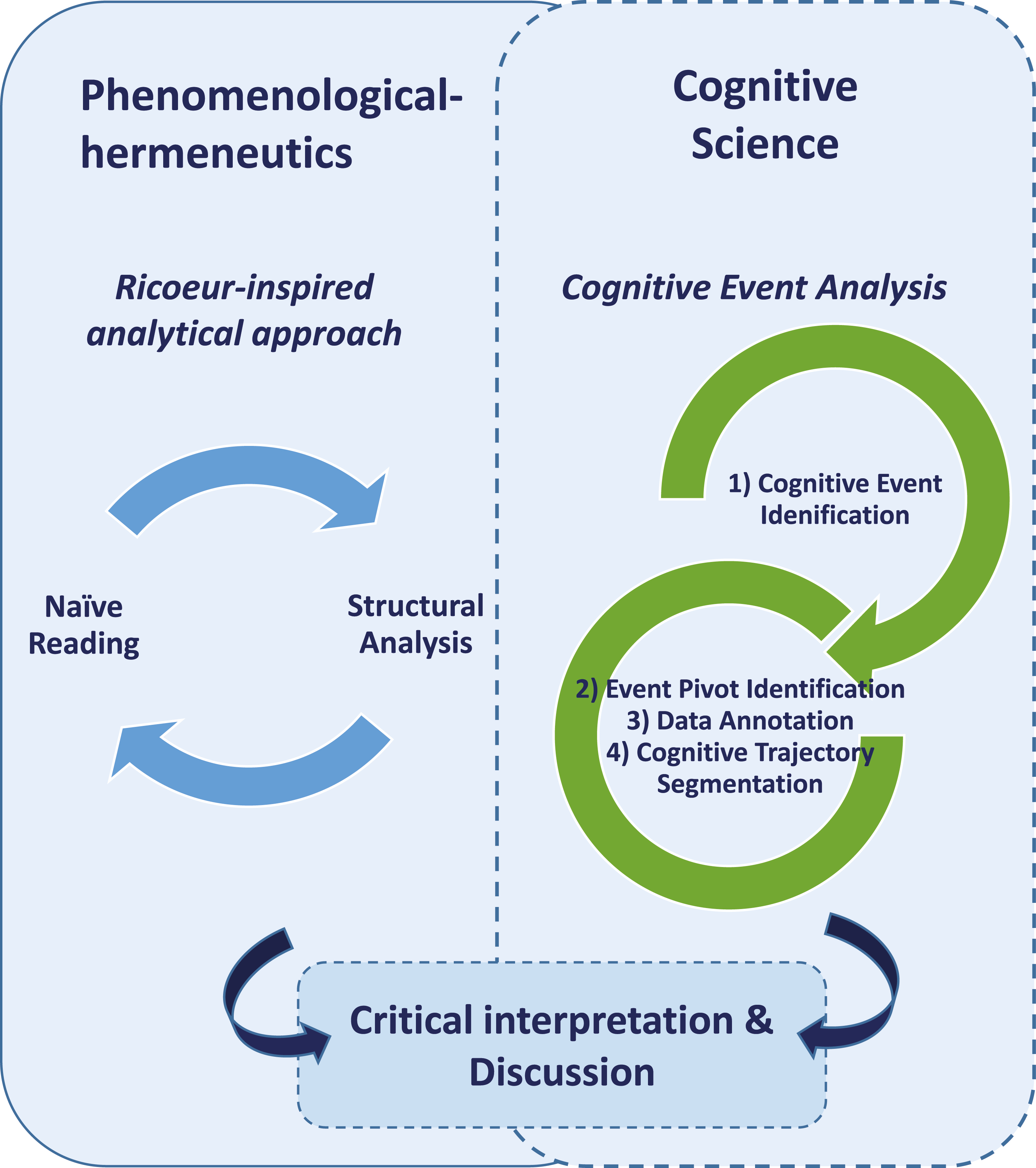
This article demonstrates a hybrid method containing a first- and third-person perspective. The hybrid comprises identifying, understanding, describing and explaining transfer of HFS into actual clinical competency. The aim is to demonstrate how the hybrid method can capture how transfer happens. The hybrid method can contribute to understanding how the participants transfer HFS from SBT to competency in everyday clinical practice. The approach (visualised in Figure 1), with both its Ricœur-inspired analysis (RIA) and Cognitive Event Analysis (CEA) of ethnographic data (abbreviated RI-CEA), illustrates how research in SBT on HFS can benefit from methods other than the typical quantitative and descriptive methods.

The hybrid method RI-CEA, a phenomenological–hermeneutic approach combined with a cognitive science approach
This article presents the hybrid method used in analysing data from a health science angle (Figure 2, the green path). The study is a health scientific substudy to SimLEARN. SimLEARN is a double PhD study with a social science angle [19] and a health science angle. SimLEARN explores how qualified in-hospital healthcare personnel transfers HFS learned from SBT to competency in everyday clinical practice at two Danish hospitals. Danish public hospitals are teaching hospitals and continuously receive newly educated healthcare personnel. SimLEARN’s joint data collection consists of ethnographic studies [20,21] of qualified healthcare personnel before, during and after an interdisciplinary in situ SBT course and followed the design shown in Figure 2. The researchers shadowed healthcare personnel with cameras. Five doctors and 12 nurses were shadowed in the clinical phase, and 4 nurses in the transfer phase. Other healthcare personnel were shadowed when they joined work with the ones shadowed. A total of 45 healthcare personnel participated in the SBT course, including doctors, nurses, nurse assistants and students; the researchers shadowed their training and debriefing with cameras.
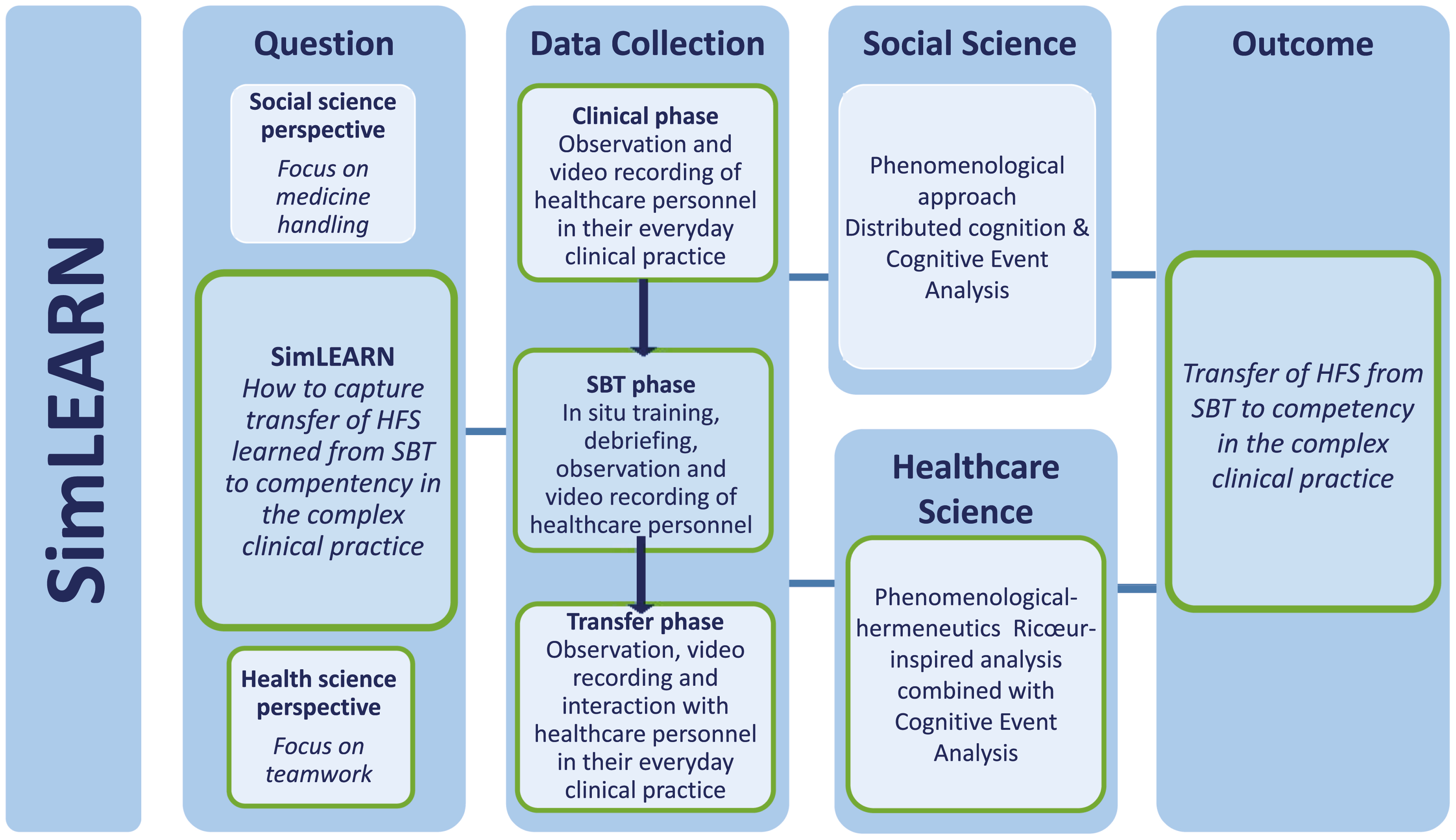
SimLEARN’s project design
Through ethnographic examples, it is demonstrated how RI-CEA deliver insights into transfer of HFS from SBT courses into the clinical every day.The Danish Data Protection Agency (ID 19/14608) and the Ethical Board of the Region of Southern Denmark (ID 20182000-140) approved the study.
The SBT course intervention in the SimLEARN study consists of introductory information meetings and a screencast about HFS to all personnel in the clinical departments before the data collection. Then 8 days of SBT and an online after-course participant evaluation survey. Each SBT day consists of three 10–20 minutes of in situ training (scenarios) at the participating hospital departments. First, a scenario about medicine room teamwork and then two patient-focused scenarios about teamwork and communication. After each scenario, a 25–30-minute debriefing [22,23] by external facilitators. The participants are volunteers at-work healthcare personnel from the duty schedule selected to match an authentic competence combination with assistance from the ward heads on the training day. All personnel can opt to decline participation, and participants give informed consent. The ethnographic data include a diverse group of clinical personnel: doctors, nurses, physiotherapists, radiologists, nurse assistants, medical students, nursing students, technicians and secretaries.
The chosen qualitative and phenomenological–hermeneutic frame is based on the French philosopher Jean-Paul Ricœur, who combined phenomenology with critical hermeneutics. Ricœur’s work bridges different philosophical positions (originating from, for example, Aristotle, Heidegger, Wittgenstein, Gadamer, Popper and Marcel) by synthesising parts into a critical phenomenological–hermeneutic philosophy [24,25].
The initial analytical approach of RI-CEA is inspired by a Ricœur-inspired approach to interpreting ways of being in the world [26–31], meaning the subjective experience of individuals and their comprehension of the lived life. The approach is created with reference to Ricœur’s writings on language, reflection and text comprehension. Healthcare researchers have extended Ricœur’s philosophy for analysing narratives, language, experiences, interviews and ethnographic data [26,27,30,32,33]. In short, humans are affected by situations and orient themselves as part of those situations (instead of behaving rationally under universal rules), which becomes their lived experience and existence in the world [3].
Observing video sequences and reading field notes as part of the RI-CEA method corresponds to how Ricœur views texts or narratives in the sense that the video sequences have left the original field and the participants with meaning to interpret. This resembles Ricœurs’ claim that a text leaves the author’s intentions. Thus, the object of study becomes the shared meaning of the video or text rather than the original intentions of the author or participants in the video. The researcher then listens to the meaning of the text and remains open to new details in video sequences or field notes for understanding, which emerge in front of the text [34,35]. Opening up the video or text through intuitive listening adds a first-person researcher’s perspective on the data and grounds the research in the interpretation process by reclaiming the field, feelings, senses and thoughts that have escaped the researcher.
As shown in Figure 3, RIA is carried out on three levels: (1) naïve reading, where the researcher notes ideas, thoughts and impressions; (2) structural analysis; and (3) critical interpretation and discussion [26,30]. The analytical process is a dialectic process moving in a hermeneutical helix between naïve reading, structural analysis, and critical interpretation and discussion. This dialectic process between parts and the whole provides an enlarged, profound and sophisticated understanding of the participants’ transformation of HFS.
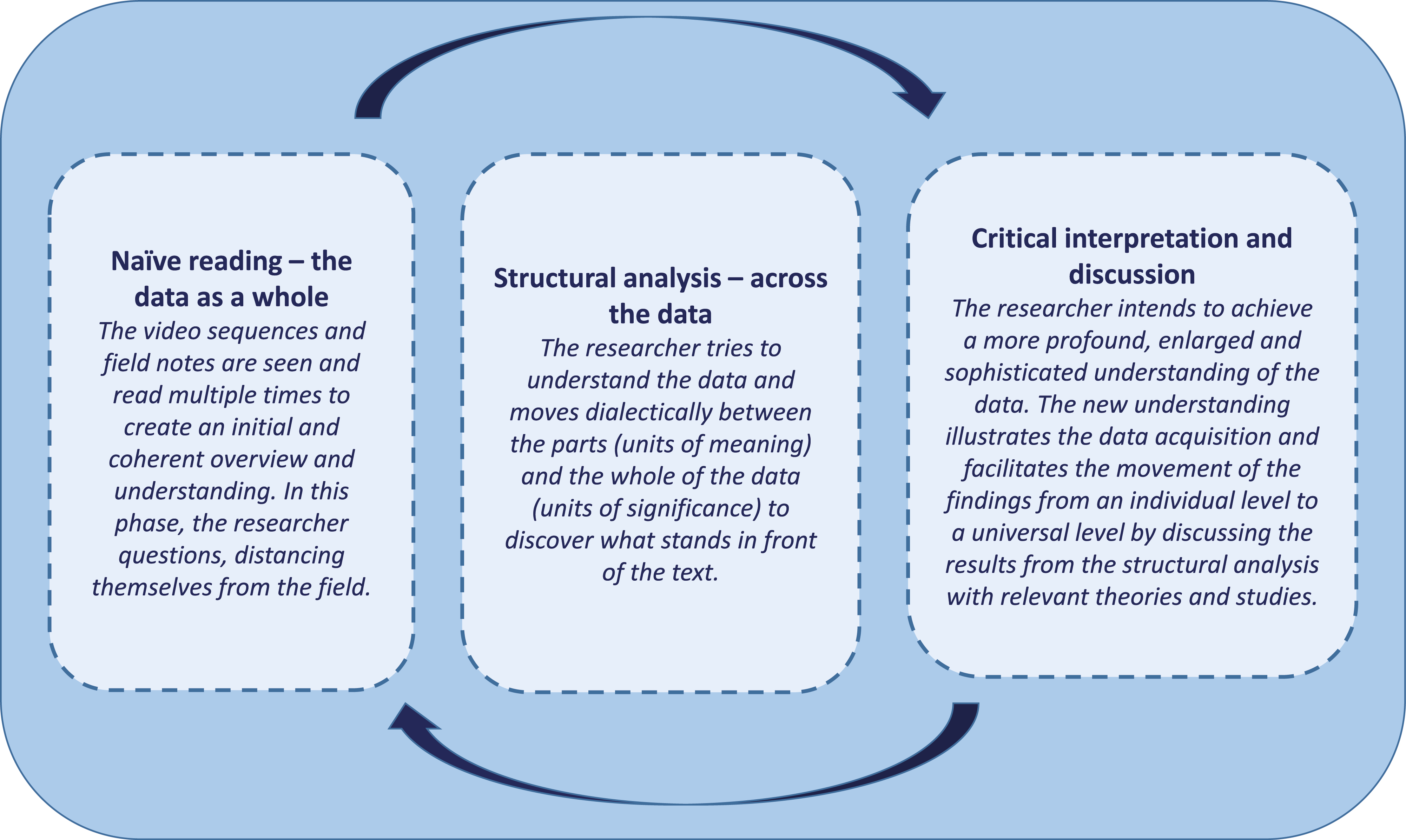
The Ricœur-inspired analytical process showing the dialectic movement between the whole and the parts
The RI-CEA method’s second analytical approach is CEA. CEA is a method with roots in cognitive science, specifically cognitive ethnography and distributed cognition [4]. Cognitive science explores thinking processes and aims to understand peoples’ thinking and behaviour by examining human tasks [36,37]. Distributed cognition is a theory with interdisciplinary roots but with a phenomenological understanding of the human as embedded in an ecology of brain, body, environment and social interactions [4,38,39]. The primary hypothesis is that cognitive processes are distributed across brain, body, environment and over time [40]. Hence, cognition is not reducible to neural function but rather distributed in a network of relations [41].
CEA is an interactivity-based method to explore cognitive processes and closely examine the bodily and inter-bodily dynamics of movements, gestures, symbols and activities. CEA builds on the thinking of Hutchins, Järviletho, Steffensen and others [4,41–44]. CEA makes it possible to zoom in and out on the organisational domain and to explore the real-time dynamics of human behaviour, where sense-making is investigated as coordination between agent(s) and an environment extended in time and space. CEA studies human cognition by focusing on bodily and inter-bodily dynamics using ethnographic video data [39]. The starting point of the CEA analysis is to identify the cognitive result (i.e. the outcome of a given cognitive process) and work backwards from this to gain insight into what caused or conditioned this result, thus gaining an understanding of the cognitive system and the cognitive trajectory [42]. To do so, CEA follows five steps:
1) Cognitive event identification: Identifying a cognitive event to further inquiry. The event is defined as a change in the person–environment system from the observer’s point of view, for example, activity of significance for the research question. The event is the bringing forth of the cognitive result.
2) Event pivot identification: Critical transition point(s) is revealed by identifying the emergence of the cognitive result and the causes and conditions that brought it forth.
3) Data annotation: The researchers annotate the data based on two independent questions: Which annotation categories does one select? And how fine-grained should the annotation be?
4) Cognitive trajectory segmentation: The researcher segments the video sequence into functionally or behaviourally defined phases by identifying annotation patterns. Having established behaviourally distinct patterns in different segments, these segments can be interpreted from a functional point of view.
5) Cognitive trajectory analysis: Finally, an interpretation of specific segments is completed based on the annotations and segmentations. The analysis identifies and explains the conditions and constraints that led to the specific cognitive results [42].
The study is divided into three steps, as shown in Figure 4. Step 1 – Clinical practice phase: It comprises ethnographic fieldwork of the qualified healthcare personnel’s HFS in the everyday. These findings’ initial analysis led to the content of the training scenarios in step 2. Step 2 – SBT phase: It comprises ethnographic fieldwork during an in situ SBT course in the included departments. The incipient analysis in step 2 led to the ethnographic focus of step 3. Step 3 – Transfer phase: The ethnographic fieldwork of the qualified healthcare personnel’s use of HFS in their practice after participating in the SBT. The ethnographic fieldwork resulted in approximately 110 hours of video data. Finally, a compiled analysis of the overall data is conducted.
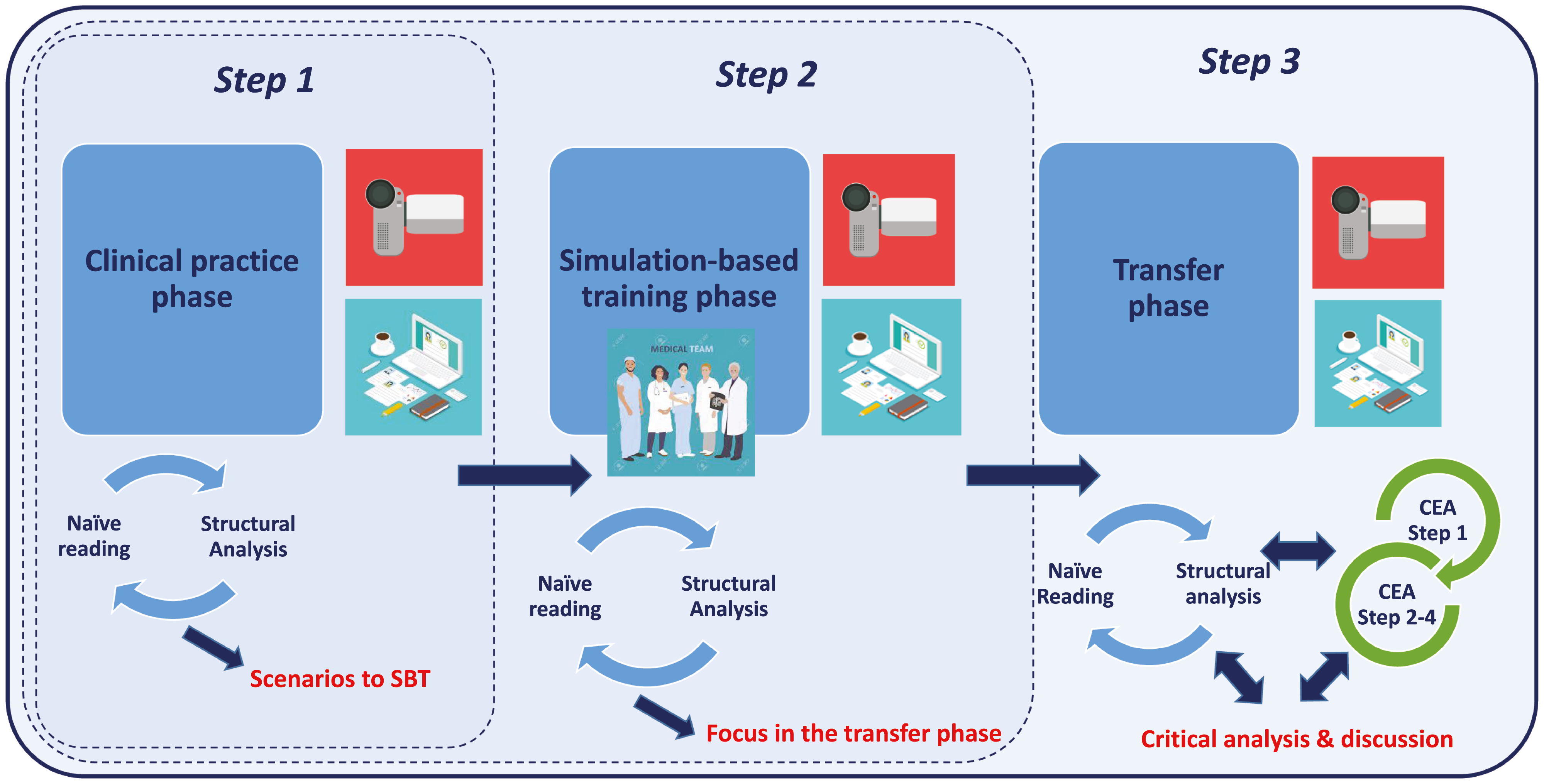
The SimLEARNS analytical process
The clinical phase comprises 2 days of ethnographic fieldwork in each participating department (Step 1, Figure 4). After the data collection, a naïve of video and field notes reading is conducted. Thoughts, spontaneous ideas, hypotheses and discussions between the two data-collecting researchers are noted and validated in the back-and-forth movement between the naïve reading and structural analysis (Figure 5a). In the structural analysis, one of the phenomena that kept appearing was different types of interruptions, which became a unit of meaning. This phenomenon was marked in the data every time it occurred. Figure 5a shows the deduced units of meaning (video descriptions, quotes or field notes), units of significance (what emerged in front of the text) and emerging themes from the analytical process (from the data to a theme).
The data suggest that personnel is interrupted often, although the types of interruption vary. The results of this initial analysis inspire the SBT scenarios, which are tailored for each participating department. The scenarios feature situations where, for example, interruptions happened, and HFS are needed for the personnel.
The SBT phase contains 2 days of SBT in all the participating departments, 8 in total. Each SBT day comprises three clinical scenarios, each followed by a debriefing (step 2, Figure 4).
After the SBT, a naïve reading and structure analysis of this phase’s data are conducted. In the naïve reading, all the data from the SBT phase are watched, read, revisited and reflected upon. Across the data, the personnel reflects on actions and responses to interruptions during the SBT, which become a unit of meaning. These reflections and reactions are marked in the data every time they occur. In the debriefing, the personnel discusses how interruptions in their workday result in stress, forgetting things, potential adverse events and changing their plans for the workday several times, among other outcomes.
The structural analysis opens a new understanding of how interruptions affect the personnel’s work. Figure 5b shows examples of the naïve readings units of meaning towards units of significance and a new understanding after the structural analysis. Data suggest again, both in the scenarios and in the debriefings, that interruptions have a strong presence in the subjective experience of the personnel, influencing their work and task completions. This analytical level identifies the focused observations in the transfer phase, looking for signs of transfer from the SBT courses.
The transfer phase comprises ethnographic fieldwork in the participating departments (step 3, Figure 4).
After collecting the final data, the total dataset is watched, read, revisited and reflected upon as a whole. A novel naïve reading and structural analysis across all data are performed. Figure 5c reflects the units of meaning (what is said, done and observed) through transcripts from the video sequences, field notes and narratives from the field observations.
RIA reveals the participants’ experiences and the researchers’ understanding. The result is what appears in front of the text. It provides a description, understanding and possible explanations of the participant’s competency development of HFS from the clinical practice phase to the transfer phase. It is, however, necessary to change the perspective to understand how this transfer of HFS happens,
CEA moves, like RIA, between the whole and the details of the video data (step 3, figure 4). Therefore, the structural analysis can be expanded through CEA, which changes the lens of the data and observes, specifically, what happens from a third-person micro-perspective. CEA begins with the emerging theme: interruptions in planned workflow from the RIAs structural analysis. The task is to explore if there are improvements in the participant’s management of interruptions from the clinical phase to the transfer phase.
Given the theme of interruptions in the planned workflow, innumerable cases are identified. Using CEA, scrutinise the cognitive dynamics of these cases. To exemplify a situation where an expert doctor (A) and a novice doctor (B) make a joint decision is chosen. A and B sit in an office, facing a computer at a long desk against the wall. B makes oral noises like sighing and heavy breathing. A looks briefly at B and asks, ‘Do you need help?’. B nods, and A rolls over to her looks at her screen, asks her some questions about the patient’s case and moves back again. They discuss different treatment and care options and make a joint decision in a complex situation. Joint decision-making is a cognitive event; the point on the cognitive trajectory in which they reach a decision is the primary event pivot. Moving backwards from the event pivot and analysing what prompted the joint decision-making, the persons’ behaviour is annotated in four area activities, gaze, vocalisation, facial expression and positioning.
Based on the annotations shown in Figure 6a1, the video sequence is segmented into seven different behavioural and functional phases. Figure 6a2 presents the trajectory segmentation, revealing that B interrupted A, not directly, by sighing and making noises to catch A’s attention. When A becomes aware of B’s sounds, A looks at B for three seconds, then rolls to B and asks, ‘Do you need help?’. B nods and becomes observably less tense. Together, they look at B’s screen, reflecting on the medical problems and discussing her treatment options, pros and cons. A supports her reflections by asking B for the most plausible solutions to treat the patient and helping her balance options and risks. The result is joint decision-making concerning the treatment of the patient.
In the vocabulary of CEA, the analysed situation occurs on two time scales: a problem-solving scale and an educational scale. The analysis reveals seven different HFS: situation awareness, leadership, followership, teamwork and decision-making. As novice doctors learn during work, a possible interpretation could be that they know that interruptions can lead to adverse events, that it is necessary to minimise these, and that expert doctors are very busy due to heavy workloads and teaching–learning situations. B might feel she ought to solve the clinical problem herself without support from an expert doctor busy with his tasks.
On the other hand, novice doctors are trainees and need help, support and educational guidance from competent and expert doctors to learn and avoid adverse events. This dilemma can be why it is difficult for novice doctors to ask for help and teaching. A used about 3 minutes to supervise and reflect with B to help her learn deductive and reasoning ways to move from a problem to a solution in the future. Although A could have provided B with the answer to her problem, A turned the situation into a learning event instead. Consciously or not, A and B work and train their HFS in this situation.
Exemplifying the CEA of the SBT phase, an acute training situation, where more qualified personnel is called to the patient room to ensure decision-making, is chosen.
The SBT scenario: A novice nurse (N1) and a nurse assistant (NA) receive an acute patient. A young woman is found outside the hospital on the pavement lying beside a bike, without a bike helmet and with scratches on her feet, arms and head. She is delirious and cannot give her full name and social security number or tell what has happened. N1 calls an expert nurse (N2) for decision support and later a doctor (D) for treatment.
Two cognitive events are identified, as shown in Figure 6b. The first is the nurses’ joint decision-making, and the second is joint decision-making between N1, N2 and D.
The behaviour mapping and segmentation produce eight functional phases (Figure 6b). In phase 1, N1 and NA measure the patient’s vital signs and blood gas and puts her on oxygen. N1 reflects out loud about the vital signs and blood gas results, but NA remains silent and unresponsive (lacking followership). In the second phase, N1 concludes: ‘I will call (phone) N2 for help’, and NA nods. N1 interrupts N2 in phase 3 when she calls her, but N2 supports N1’s need for backup. In phase 4, when N2 arrives, N1 summarises the situation, repeats her reflections and presents N2 with the blood gas results. N2 reflects with N1 and concludes that the patient has a low glycaemic index and needs a doctor to prescribe the dose and volume. In phase 5, N1 calls D and interrupts her in her rounds. In phase 6, N2 send NA after the glucose fluid, almost simultaneous with N1’s call to the doctor. When D arrives in phase 7, N1 resumes the situation and repeats their (N1, N2) reflections and the low glycaemic index. D takes the lead but includes N1 and N2 in joint decision-making. At the same time, NA re-enters with the glucose fluid, and N2 is ready to connect it to the patient as D prescribed it.
The analysis suggests that six different HFS come into play: situation awareness, leadership and followership, teamwork, coordination, and decision-making. Similar to the clinical phase example, two different time scales are integrated with clinical behaviour: problem-solving and educational scales. A possible interpretation could be that N1 might experience insecurity and acknowledge that she lacks competencies. She receives no support from NA, so she calls for help from a more expert co-worker. N2 is an expert and, apparently, used to guide, teach and support novices, and due to this, she does not take the lead, although N2 evidently, has experienced this situation before and knows the algorithm. N1 keeps the leadership, and N2 provides support and followership. N2 supports N1 in becoming a competent nurse to trust her competencies and decisions. In this way, the situation turns into a clinical and educational situation, where they treat the patient simultaneously as N1 learns to cope with this acute situation.
When the facilitators ask about the authenticity of the situation during the debriefing, the team recounts the everyday needs for support, teaching and learning. The team underpin that this need results in many interruptions of the expert personnel. The SBT team also concludes that these interruptions are unavoidable. Through the reflections, the team reaches the new understanding that it is okay to interrupt when one needs help, but one must do it with circumspection. The SBT team become aware of the influence of interruptions on the workflow and patient safety. Interruptions per se might be unavoidable. Still, a decrease is necessary, as some interruptions are required, but others can be avoided. Sometimes the personnel are more focused on delivering the messages to their colleagues – getting the information out of their heads – than on the interruption problem. The team concludes that they can limit interruptions.
An event where two nurses pass each other in the hallway exemplifies using CEA to study interruptions in the transfer phase.
N2 (expert nurse) walks towards the nurse station when she meets N1 (competent nurse) in the hallway. N1 looks at N1 and sends N2 a tiny smile. N2 lowers her walking speed. N1 stops, and N2 joins. N1 initiates the talk; she needs help. They both outline their planned tasks and coordinate these. In this situation, three events are identified: (1) an unplanned coordination and decision-making, (2) a sudden unintended joint care for a moaning patient, and (3) a joint decision to change plans again.
As shown in Figure 6c, a moaning patient catches their attention and interrupts their coordination. With brief eye contact, they change their plan and enter the patient’s room. Back on track, they meet the husband, whom the nurses know cannot speak with his demented wife, so they inform him of the current situation.
The mapping and analysis of the event (Figure 6c) result in nine different behavioural and functional phases where four different HFS come into play: situation awareness, teamwork, coordination and decision-making. In phase 1, N1 stops N2 with eye contact and a smile; she needs help. In phase 2, the nurses plan and coordinate their tasks when they hear a moaning patient nearby. In phase 3, N1 and N2 look briefly at each other, turn around and enter the room to care for the patient. Later, in phase 5, the patient’s husband arrives on their way to the planned joint task. The husband looks at N2 and smiles. In phase 7, N2 gazes briefly at N1, then back at the husband, stops and informs him. N1 waits silently at N2’s side. The nurses are once more interrupted in their plans. They prioritise informing the relative before they continue with the planned tasks. This decision is hypothetically reached through eye contact and smiles.
A possible interpretation is that the meeting in the hallway allows N1 to ask for help with a tiny smile. N2’s action of slowing down her speed could be her reaction to N1’s smile and nod and signal to N1, You can interrupt me. In the same way, they communicate silently and with their eyes and smile when they choose to take care of a moaning patient and, later, her husband. The nurses demonstrate a kind of interruption readiness. Based on the nurse’s knowledge of the patient, they prioritise caring for her before their planned tasks. They do not decide with words, but with a glance at each other. It is plausible to say that the nurses use their HFS and tacit knowledge both when interrupted and when they make quick decisions and change their plans from the original due to new unplanned situations. Although they had other plans, they changed them due to the needs of the present situation.
The final step of RI-CEA is a critical interpretation and discussion of the results from the analytical processes (step 3, Figure 4). The parts (units of significance and themes from RIA and CEA analysis) are gathered and critically interpreted. In the critical interpretation and discussion, the researcher intends to achieve a more profound, enlarged and sophisticated understanding of results, their validity and generalizability. The new understanding illustrates the data acquisition and facilitates the movement of the findings from an individual level to a universal level by discussing the results with other relevant theories and studies [3,26]. In discussing the results, the overall results are reviewed and then validated by asking if these results are plausible in light of the whole SimLEARN dataset and research question regarding transfer of learning. Is it conceivable that SBT of HFS can develop the personnel’s awareness of interruptions and begin changing their articulation and behavioural actions in everyday practice? And if yes, how did this transfer happen? This validation is then discussed by including relevant literature about the effectiveness of SBT, re-learning, development of new skills, and transfer of learning. Secondly, the generalizability of the results is appraised by considering if the results can be universal or not.
Two themes emerged from the analytical process: interruption readiness and clinical education. In some ways, these themes are intertwined in daily practice. The Danish hospitals’ constant flow of newly educated personnel, as well as a high personnel turnover, creates a need for continuous learning; the expert personnel must support, guide, teach and educate the novices to cope in a complex shifting practice with high emotional demands. In addition to pursuing tasks, the expert personnel must develop an interruption readiness to cope with the inevitable interruptions from younger colleagues. One can wonder why this interruption readiness skill is not a focus when introducing or training newly educated healthcare personnel. The results show how the healthcare personnel, through SBT, become aware of the importance of HFS competencies to cope with interruptions in their everyday clinical practice [45]. Data indicate a change in the personnel’s awareness, talk and considerations about interruptions.
The outcome of the HFS training is learning on an individual level and not changing the local organisation’s way of working with interruptions. This might be due to the researchers’ lack of emphasis and unclear feedback to the department managers regarding the need for subsequent implementation of the SBT outcome, continual focus on interruptions and the importance of the interruptions for the novices learning, the experts’ workflow and patient safety. Comparing possible changes through SimLEARNS’ three phases (clinical, SBT and transfer), it is conceivable that the SBT focusing on interruptions can have changed and articulated some participants’ behaviour around interruptions.
The research question’s transfer perspective requires more than understanding and explaining how humans develop competency through educational interventions. RIA offers insight into the personnel’s being in the world. CEA provides a change of lens on data from what emerges in front of the text (RIA) to an analysis of the personnel’s cognitive changes (CEA) during and after the intervention.
Expanding RIA with CEA in a phenomenological–hermeneutic frame gives a broader picture of how healthcare personnel transfer HFS from SBT to competency in the everyday are gained. RIA investigates the understanding and explanation, whereas CEA investigates the how based on real-time dynamics and non-local conditions. The structural analysis clarifies that RIA cannot answer how transfer happens independently. A need to understand not only if transfer happens but also how transfer occurs; the CEA add-on is necessary to gain insight into the how. The SimLEARN case shows that integrating CEA in RIA’s structural analysis broadens the analytical outcome and expands the research outcomes to a strengthened result. The CEA microlens perspective on the cognitive and real-time activities enhances the validation step of RIA.
The two methods complement each other and expand the analytical result of the ethnographic data. Both methods progress in movements between parts and whole, and between understanding and explanation, and in that way, complement each other. CEA works with the processes that occur in the interbody dynamics, whereas RIA offers the personnel’s understanding and transformations across the three phases. This can show how cognitive processes present themselves in normative, structural and synchronic interbodily dynamics, which more traditional approaches in healthcare sciences cannot reach. The RI-CEA method is time consuming – more than 100 hours of video, field notes and self-reflection. Therefore, RI-CEA might not be the preferred method to confirm transfer. However, it can broaden the insight into the phenomena of transfer and be the foundation to develop a more useable and accessible approach to grasp transfer of HFS.
The theoretical and practical combination of analysing the data opened up the data to what was going on, what it was about, how did the personnel function and behave and did it change practice. The lived experiences of the qualified personnel during and after an SBT course reveal and confirm if HFS is transferred to everyday clinical practice. This lens shift adds an in-depth picture of the personnel’s behaviour and possible behavioural changes in HFS skills after SBT. For instance, where a competent and an expert nurse meet. N1 gazes and smiles at N2, and N2 reduces her speed. This could indicate N1’s new competency in reading N2’s interruption readiness. When N2 reduces her walking speed, N1 initiates a talk and expresses her need. Expanding RIA with a CEA, a hybrid method has been designed, containing approaches which might give insight, understanding and explanation of transfer.
The hybrid method with RIA and CEA can capture transfer. The hybrid method expands the existing insight into how and if transferring human factor skills after simulation-based training becomes competency. By observing the data closely, the personnel’s performance becomes visible, and it is possible to train towards a desirable goal (e.g. manage interruptions) and, through in-depth analysis, perceive how the personnel gains a new language around interruptions, and for some personnel changed behaviour. However, this hybrid method is time consuming and needs further development and evaluation.
A few limitations of this description of the hybrid method must be highlighted. Firstly, the hybrid method is experimental in an ongoing project, and the final results still need to be done. The researchers tried to meet this challenge by unifying experts in both project methods (healthcare science and social science). This allowed the researchers to reflect on and discuss this hybrid method’s pros, cons and extent. Secondly, the department leaders pointed out the participants, which could influence the psychological safety issue. However, all participants were allowed to decline participation. The course was not mandatory, and therefore, is a positively biased result possible because the participants had accepted SBT as a learning method [46] and possibly wanted the study to succeed. The researchers tried minimising this limitation by selecting the participants on the day within the group of staff on duty. Finally, there is a risk of observer bias, a systematic variation in the observations [46], which can reduce the hybrid method’s applicability. This could have contributed to concluding transfer where there was none, but instead a coincidence. Nevertheless, video analysis makes it possible to revisit the situations, behaviour and responses from the participants and field notes multiple times, reflect and discuss these in the researcher group to validate the findings.
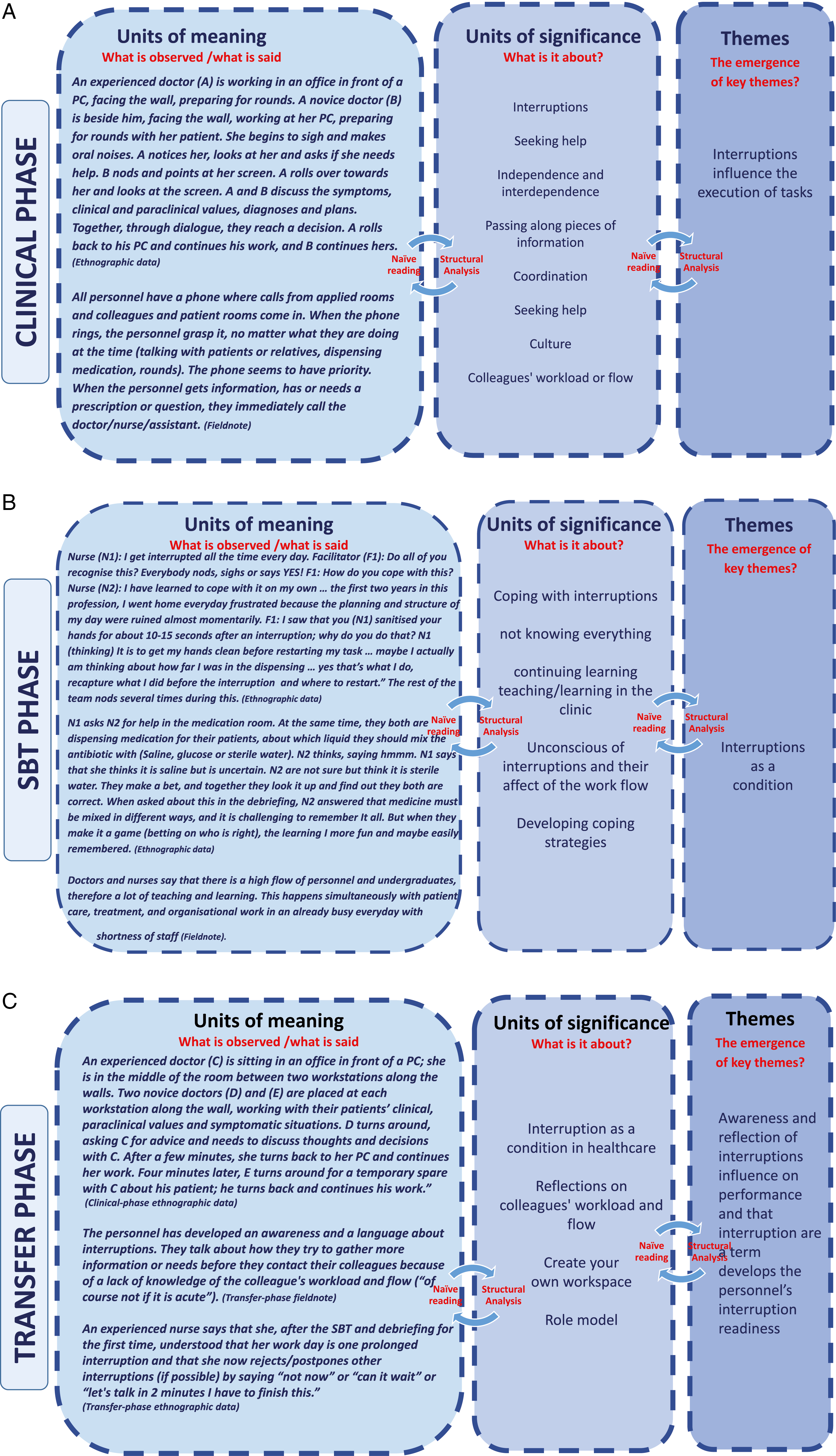
(A) The analytic process from naïve reading to the structural analysis of the clinical phase. (B) The analytical process from naïve reading to the structural analysis of the SBT phase. (C) The naïve reading and the structural analysis of the overall data. A shows the analytical process in the clinical phase, B in the SBT phase
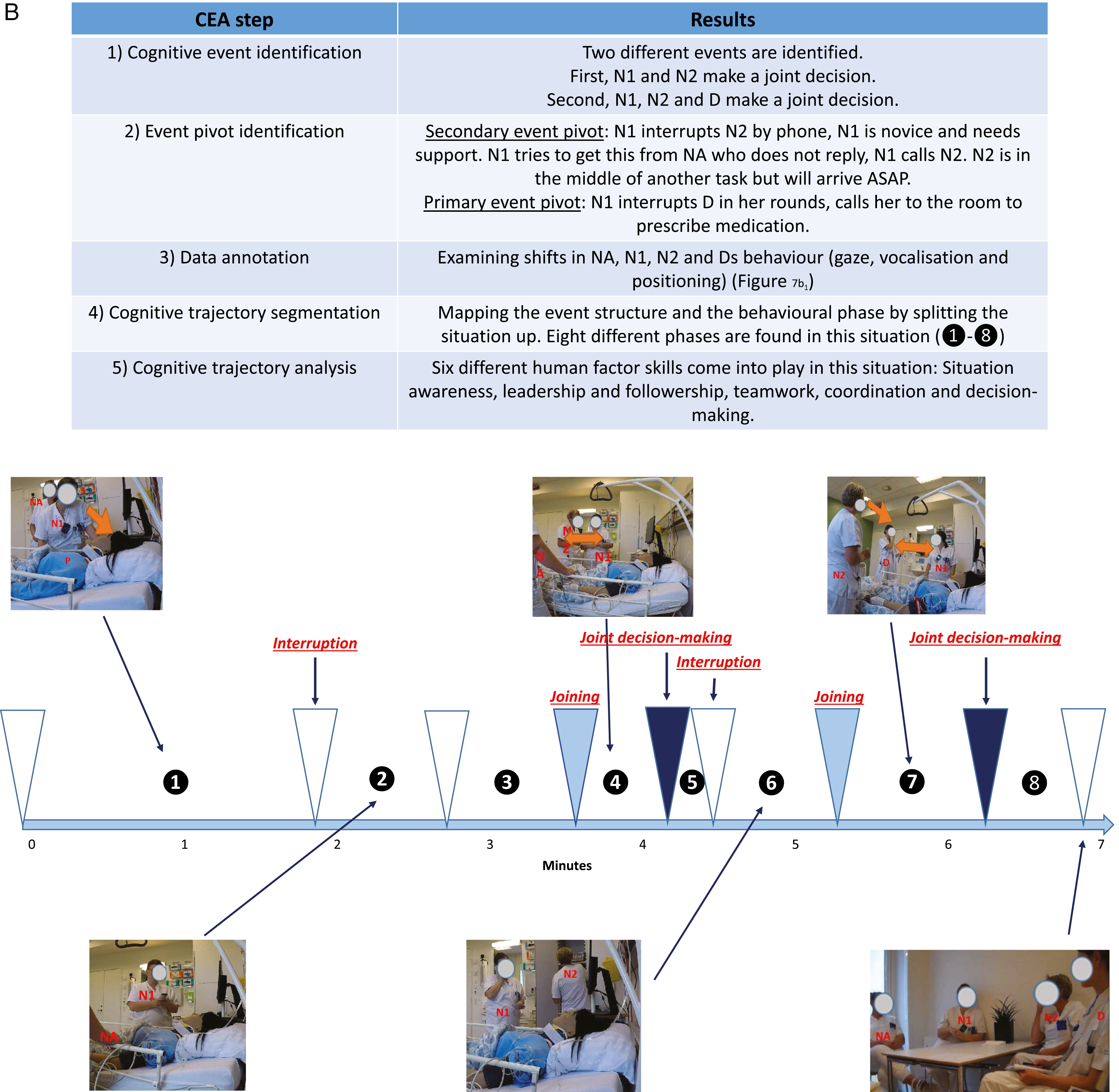
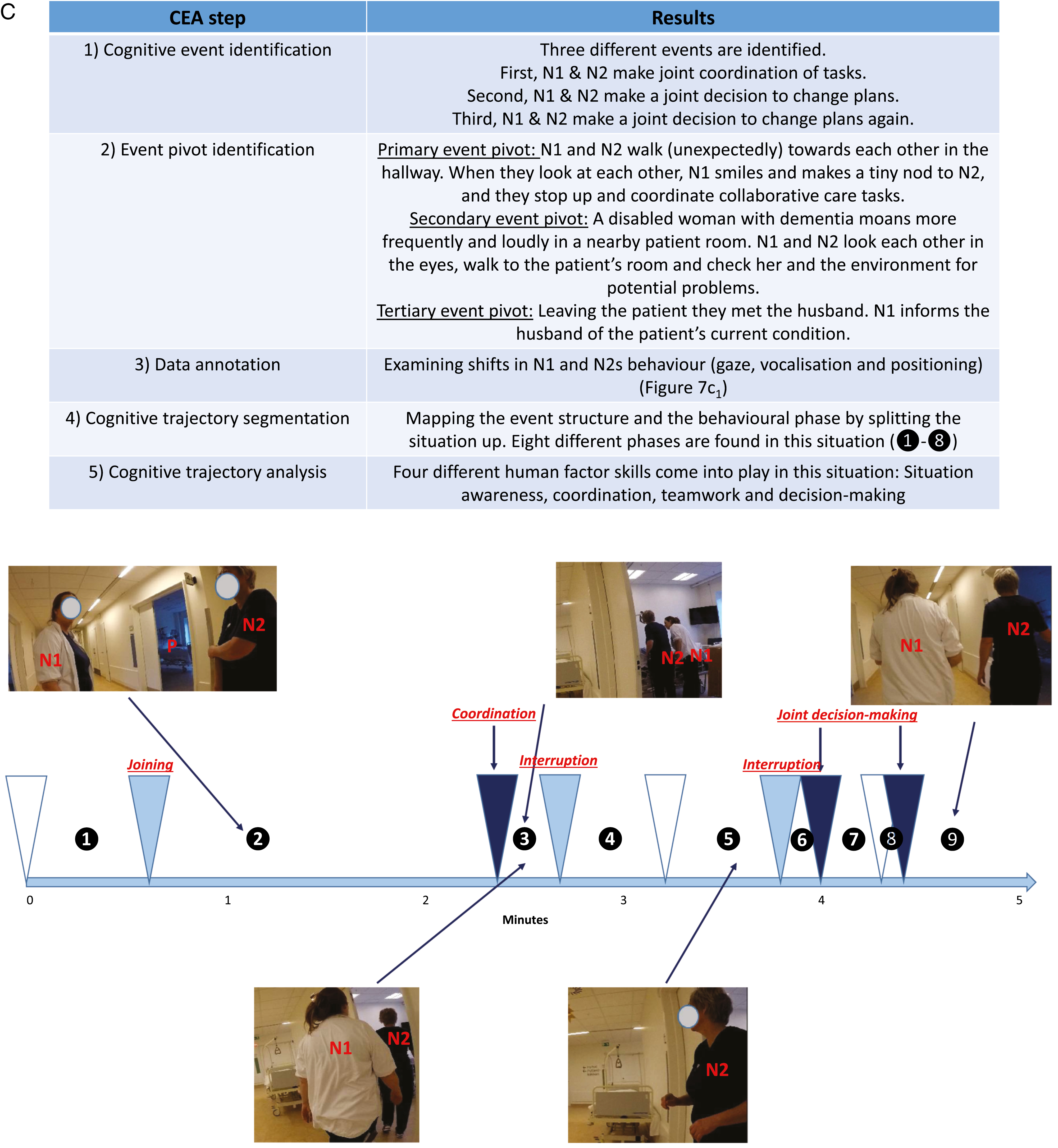
Note to Artwork: Missing figure 6a1 and 6a2. There should be 3 parts of CEA analysis, right now there are 2 parts. The annotation figure are only present for the first CEA analysis, that means that 6a1 are different from the other figures in figure 6. Sorry I know its big data. (a1) Data annotation of activities, phases and behaviour. (a2) Cognitive Event Analysis with microlens interpretation of interruptions. (B) Cognitive Event Analysis of interruption in the simulation-based training phase. (C) Cognitive Event Analysis of interruption in the transfer phase
Lotte Abildgren drafted the article. All authors critically revised the manuscript and the authors read and approved the final manuscript.
Anesthesiology and Intensive Care Department V, Odense University Hospital, Denmark, Department of Clinical Research, University of Southern Denmark & Hospital Sønderjylland, Aabenraa, Denmark.
None declared.
None declared.
None declared.
1.
2.
3.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
 Transfer of human factor skills from simulation-based training to competency in clinical practice – a demonstration of a hybrid method for assessing transfer of learning
Transfer of human factor skills from simulation-based training to competency in clinical practice – a demonstration of a hybrid method for assessing transfer of learning
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets