
Reduced clinical placement capacity, the COVID-19 pandemic and growing training place numbers have resulted in the development of innovative placement design in healthcare education. Simulation is widely used in healthcare education; however, its use as a placement model is in its infancy. The experiences and perceptions of students and educators are important to shape simulated placements moving forward.
A systematic search of the literature was conducted on eight databases to identify qualitative and mixed-methods studies exploring the experiences of students or educators in the nursing and allied health professions. Eight studies met the inclusion criteria and were assessed for methodological quality using the Joanna Briggs Institute (JBI) critical appraisal checklist for qualitative research. A meta-aggregative approach, in accordance with JBI guidelines for reviews of qualitative evidence, was used to synthesize the results.
From the eight studies, a total of 69 findings were extracted. These were grouped into nine categories to form three synthesized findings of overall low quality. These findings were related to (1) reality of the simulated placement, (2) emotions evoked during the simulated placement, and (3) opportunities and challenges associated with implementing simulated placements.
Simulated placements were considered a useful tool for the enhancement of communication skills, clinical reasoning skills, new knowledge generation, enhancing reflection and for preparation for clinical practice by students as well as educators.
What this study adds
Practice-based learning is the cornerstone of healthcare education. In the United Kingdom, there are a range of hour-based stipulations that need to be completed pre-qualification. Growing workforce demands have driven an increase in training places. A significant barrier to increasing student numbers is the provision of clinical, patient-facing placements. Simulated placements (SimPs) have been used to increase capacity [1]. Lasater [2] suggests that up to 25% of standard placement provision can be replaced by simulation without detriment to student performance.
Gaba [3] defined simulation as ‘a technique used to replace or amplify real experiences with guided experiences that evoke or replicate substantial aspects of the real world in a fully interactive manner’. In the physiotherapeutic context, a form of low-technology simulation is routinely used in classrooms, where students practise therapeutic skills such as mobilization techniques or electrical stimulation on their peers in a clinic-like setting. However, the use of simulation in delivering clinical physiotherapeutic placements is relatively new and the literature is sparse [4].
Pears et al. [5] suggest that innovation in placement models has accelerated in response to staff redeployment and social distancing due to COVID-19 and increasing student numbers. This has forced institutions and educators to rethink the delivery of clinical education without compromising the quality of training. A range of models have been trialled including campus-based, pre-clinical and speciality-specific placements [2].
The major advantage of SimPs over clinical placements is the opportunity for deliberate practice [6,7] where clinical scenarios are curated for skills acquisition rather than the unpredictability of a clinical placement environment where learning is subject to patient availability. A systematic review by Mori et al. [8] of 23 quantitative papers in physiotherapy entry-to-practice curricula concluded that simulated learning benefits students by enhancing learning, clinical reasoning and skills development whilst simultaneously reducing placement-related anxiety The evidence on simulation effectiveness in healthcare education is extensive, but low in quality [9], while evidence on students’ or educators’ experiences is sparse. This qualitative systematic review aims to explore the experiences of allied health and nursing students and educators of SimPs.
This qualitative evidence synthesis (QES) was conducted and reported in accordance with JBI guidelines for QES and PRISMA reporting guidelines [10]. Meta-aggregation was used to synthesize the results. This approach seeks to create generalizable statements which can be used for developing recommendations to guide practitioners and policy-makers [11].
Nine databases were searched, of which five were healthcare databases (CINAHL, Medline, PubMed, SCOPUS and Web of Science) and four educational (British Education Index, Emerald, ERIC and Proquest Education database). A scoping review of Medline confirmed that simulated placements have been incorporated into nursing curricula since 2002 and therefore databases were searched from 1 January 2000 to 20 September 2022 [10]. Key concepts for the search strategy were students and educators in allied health professions (AHP) or nursing; simulated or virtual placements; and experiences. The final search strategy can be found in Supplementary Appendix 1. Alterations to the search strategy were made as necessary for each individual database. Reference lists of included studies were hand searched for additional eligible studies.
Studies were included that (1) were peer-reviewed primary qualitative or mixed-methods studies; (2) investigated AHP and nursing bachelors and masters level students and educators; (3) investigated SimPs where they were designed to replace standard clinical placements in healthcare settings; and (4) recorded experiences of students and/or educators following involvement in a SimPs. Studies were excluded if they were primary quantitative studies, reviews, unpublished studies, conference proceedings or abstracts; investigated medicine and dental healthcare settings; were published in languages other than English or focused on simulation as a replacement for classroom-based teaching. Studies that recorded experiences following just a single simulation session were excluded.
Two reviewers (KS, CM) independently screened titles and abstracts followed by screening of full-text articles using the eligibility criteria. Conflicts were resolved through discussion between the reviewers, and continuing conflicts were resolved through a third reviewer (KSt).
Quality assessment was undertaken by two reviewers (KS, CM) using the 10-item JBI critical appraisal checklist for qualitative research (JBI-QARI) [12]. Reviewers’ discrepancies were discussed until a consensus was reached. A third reviewer (KSt) was available to resolve the remaining conflicts. Each study was graded for dependability against 5 of the 10 JBI-QARI items. Initially, each study was considered to have high dependability. Where a study had a score of 4 or 5, dependability remained unchanged. Studies scoring 2 or 3 were downgraded by one level (moderate dependability) and those scoring 0 or 1 were downgraded by two levels (low dependability). No study was excluded on the basis of poor quality as suggested by Thomas and Harden [13]. Agreement between reviewers for screening and methodological quality was assessed using Cohen’s kappa statistic. A kappa value between 0 and 0.2 represents slight agreement, 0.21–0.4 represents fair agreement, 0.41–0.6 moderate agreement, 0.61–0.8 substantial agreement and 0.81–1 almost perfect agreement [14].
Qualitative data were extracted from studies by two independent reviewers (KS, CM) using a standardized data extraction tool (JBI SUMARI). The data extracted included details about population, context, culture, geographical location, study methods and phenomena of interest. Findings and their illustrations were extracted verbatim and assigned a level of credibility: Unequivocal (U), Credible (C) and Not-Credible (NC). A finding was deemed credible if it had at least one supporting illustration and non-credible if there was no supporting illustration. The two reviewers reached consensus through discussion with disagreements being resolved through a third reviewer (KSt). Qualitative research findings were aggregated after credibility was established [12]. This involved categorizing research findings based on similarity in meaning. These categorized findings were then grouped to produce a single comprehensive set of synthesized findings. Each synthesized finding was assigned a dependability rating based on the dependability of its constituent studies. The dependability of synthesized findings remained unchanged if constituent findings were unequivocal, downgraded by one level if the findings were a mixture of unequivocal and credible findings, and by three levels for a mixture of credible and non-credible findings.
After searching all databases, 10,958 hits were obtained. Twenty-nine studies were considered for full-text scanning and eight studies were included in the review (see Figure 1).

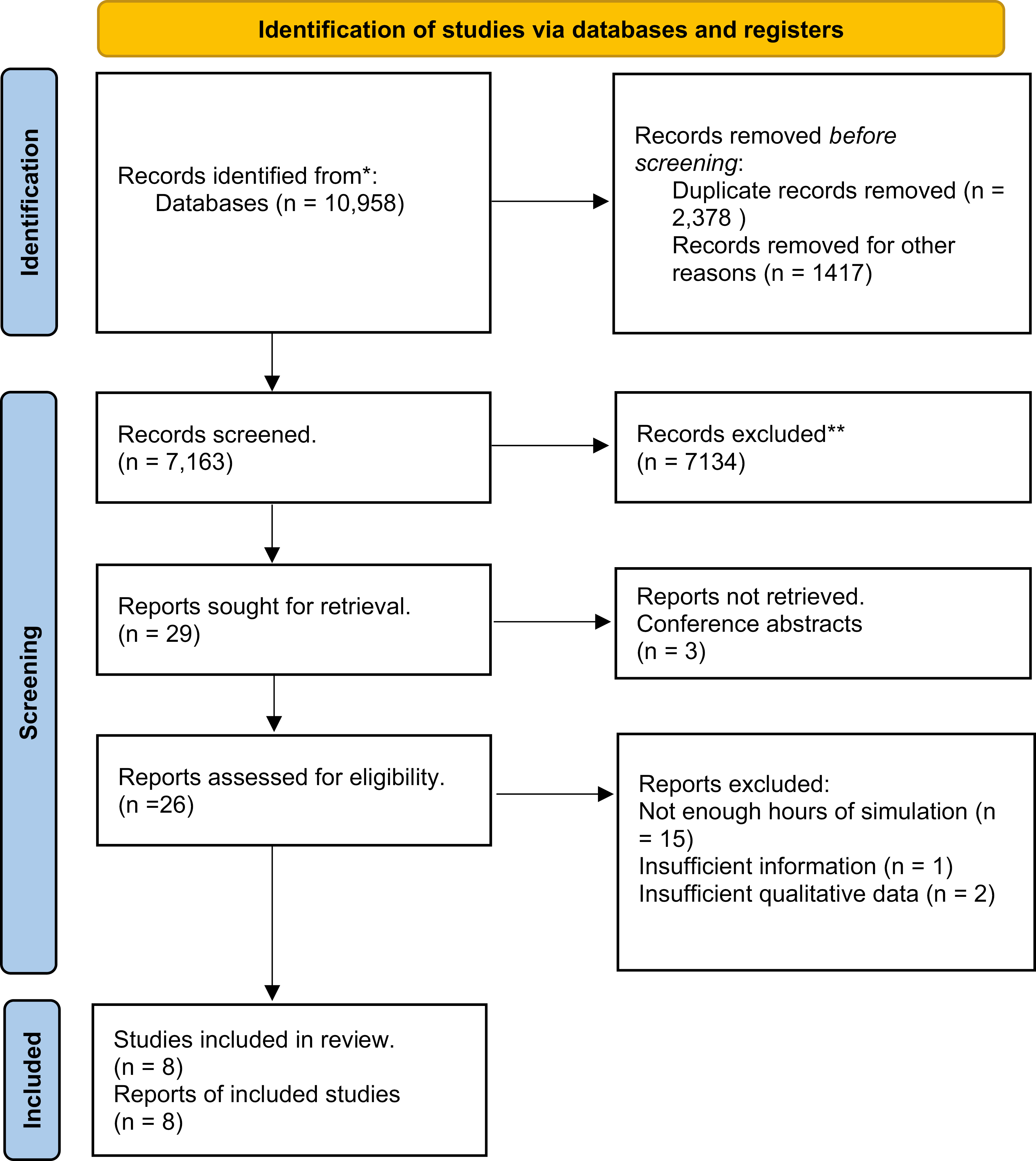
PRISMA flowchart of screening process
Study characteristics are reported in Table 1. The studies were published between 2015 and 2021. Study settings varied with one study each from Madagascar/Tanzania, Qatar, Italy, Spain, UK, USA, Canada and Australia. Participants ranged from 6 to 101 and simulation hours ranged from 8 to 84 hours over the course of 3 years. The studies were conducted within nursing except for one investigating speech and language therapy [15–17]. Simulation types were homogenous and included mannequins, role-play or standardized patients (SP). One study used a computer-based application for delivering virtual online placements [15]. Data collection methods included focus groups (n = 5), interviews (n = 2), reflective journal entries (n = 2) and recorded debriefing sessions (n = 1). Methods employed for data analysis included thematic (n = 3), content (n = 2) and interpretive phenomenological analysis (n = 3).

| Study. no. | Title | Authors | Year of publication | Study setting | No. of participants | Population | Type of simulation | Hours of simulation | Method of data collection | Method of data analysis | Methodology and philosophical background |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Nursing students experiences with simulation-based education as a pedagogic method in low resource settings-A mixed-method study | Bø, Bodil; Madangi, Bartholomayo Paulo; Ralaitafika,Hanitra; Ersdal,Hege Langli; Tjoflåt, Ingrid | 2021 | Rural Tanzania and Madagascar | 99 | Nursing students | Role-play | 9.5 | Focus groups | Content analysis | Descriptive |
| 2 | Simulation as a Disruptive Innovation in Advanced Practice Nursing Programs: A Report from a Qualitative Examination | Campbell,Suzanne Hetzel; Nye,Carla; Hébert, Susan Henley; Short,Candice; Thomas,Marie H. | 2021 | USA | 15 | Nursing faculty | Unclear | Unclear | Focus groups | Thematic analysis (disruptive innovation theory) | Phenomenology |
| 3 | The lived experiences of intensive care nursing students exposed to a new model of high-fidelity simulation training: a phenomenological study | Dante,Angelo; Masotta,Vittorio; Marcotullio,Alessia; Bertocchi,Luca; Caponnetto,Valeria; La Cerra,Carmen; Petrucci,Cristina; Alfes,Celeste Marie; Lancia,Loreto | 2021 | Italy | 15 | Nursing students | High fidelity | 8 | Interviews | Interpretive phenomenological analysis | Iterative interpretive approach |
| 4 | Practising on plastic people: can I really care? | Dean, Sue; Williams, Claire; Balnaves, Mark | 2015 | Australia | 8 | Nursing students | High fidelity (mannequins) | Multiple encounters throughout 3 years of degree | Focus groups | Thematic analysis | Case study |
| 5 | Motivation: bringing up the rear in nursing education. Motivational elements in simulation. The participants’ perspective | Díaz-Agea, J., Pujalte-Jesús, M., Leal-Costa, C., Gargía-Méndez, J., Adánez-Martínez, M. & Jiménez-Rodríguez, D. | 2021 | Spain | 101 | Nursing students | High fidelity (mannequins and SPs) | 100 h during their degree | Focus groups | Content analysis | Grounded theory and interpretivist paradigm |
| 6 | Male nursing students’ experiences of simulation used to replace maternal–child clinical learning in Qatar | Kennedy, D., Jewell, J & Hickey, J. | 2019 | Qatar | 10 | Male nursing students | Mod to high fidelity simulators, role-play, case studies, task-training and SPs | Not specified but an entire clinical course so probably multiple sim experiences | Recorded debriefing sessions and reflective journals | Thematic analysis | Qualitative approach |
| 7 | How was it for you? University practice educators’ reflections on delivering a creative clinical placement during COVID-19 pandemic in the UK | Parrott, L., Pettit, E., Mallinson, A., Knox,P., Bates, S. & Callard, J. | 2021 | UK | 6 | Speech and language pathology staff | Computer simulated learning envy (Simucase®) | One day a week across 7 weeks | Written reflections | Interpretive phenomenological analysis | |
| 8 | Caring values and the simulation environment: an interpretive description study examining select baccalaureate nursing students’ experiences | Thorp, L. & Bassendowski, S. | 2018 | Canada | 16 (10 + 6) | Nursing students | Medium fidelity mannequins | 84h throughout one year | Focus groups and semi-structured interviews | Interpretive Phenomenological Analysis |
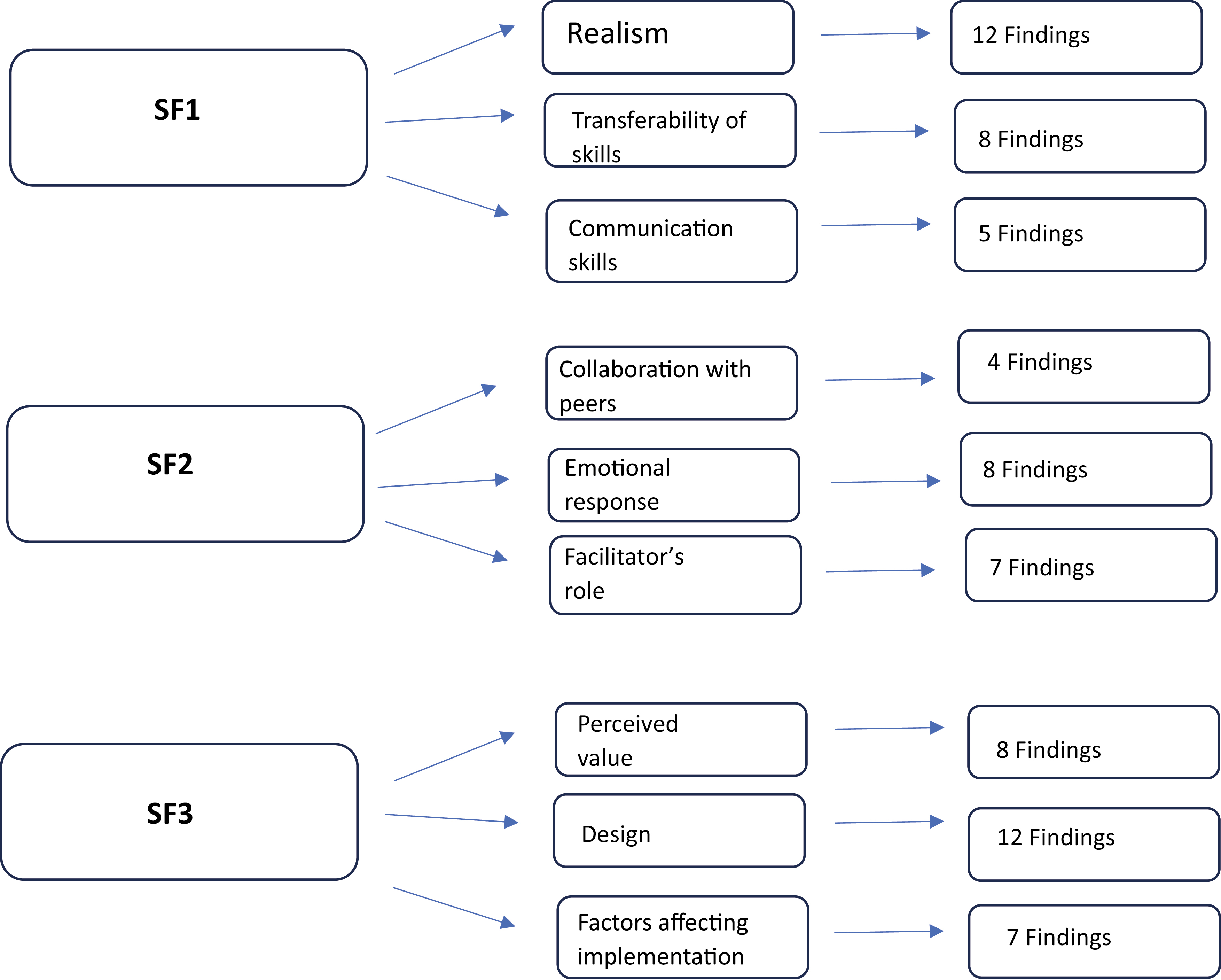
A total of 69 findings were extracted from the included studies, grouped into nine categories, and summarized in three synthesized findings (see Figure 2, Table 2). For tables of findings and illustrations, categories and synthesized findings, dependability ratings, and conQual analysis tables, see Supplementary Appendix 2.
| Synthesized finding | Type of research | Dependability (step 2A) | Credibility (step 2B) | ConQual score |
|---|---|---|---|---|
| Students preferred the use of standardized patients in simulation as it improved the ‘realness’ of the situation as the verbal and non-verbal feedback was much appreciated by the students and considered important by educators. Students acknowledged the importance of simulated placements as preparation for clinical practice for the development of knowledge, clinical judgement, communication skills as well as safe practices while putting theory to practice. | Qualitative | Downgrade by 1 | Downgrade by 1 | Low |
| While students expressed feeling vulnerable, exposed, anxious and embarrassed due to the newness of the experience and pressure of being judged by peers, an emotional progression from negative to positive was reported following repeated exposure in a safe environment. The facilitator played a vital role in influencing the idea of simulation by being discreet rather that authoritative and helped in developing the abstract values of caring and empathy. | Qualitative | Downgrade by 1 | Downgrade by 1 | Low |
| It was a consensus from students that repeated exposure to simulation enhanced confidence from repetition of technical skills over interpersonal skills. It provided access to a ‘forbidden world’. Educators designed the simulated placements to bridge gaps in knowledge while also acknowledging the various intrinsic and extrinsic challenges to implementation. | Qualitative | Downgrade by 1 | Downgrade by 1 | Low |
Meta-aggregative flowchart
Finding 1 encompassed three categories: realism, skills transferability and communication skills.
Participants expressed concerns about the level of realism within SimPs. Students preferred the use of SPs, with feedback from SPs feeling more real, increasing motivation to participate. Mannequins were considered inferior. Due to the lack of body language students found it difficult to behave compassionately towards an inanimate object; Emotions are non-existent because it’s a mannequin … and you can’t get what you get from a real person (S4). An educator pointed out that students would (not) be getting feedback from the client and carer in terms of how they responded…. anything that comes from the client... is really powerful learning (S6). Some students found that they grew attached to mannequins with one student saying, The more time you spend in those rooms... [the] more attached to the mannequins [we’ll get] (S8). The opportunity to work on multiple skills with the mannequins allowed some students to feel meaningfully engaged with simulation; ...each simulation made me really feel like donning the uniform, knowing that we were learning what was needed… (S5). Previous real clinical exposure enabled students to better relate to simulated patients and be more natural with mannequins: With more actual clinical experience it’s easier to try and apply to the case studies we use but without real clinical experience we can’t make it seem real (S4).
SimPs were seen as an opportunity to develop clinical competencies that prepared students for success in clinical practice: This will help us to know our competence before going to the patients(S1). They tested clinical judgement, allowing students to remember and apply theory to practise without the high stakes of a clinical placement: my experience is that after I read the theory, I have to practise, so that the knowledge will stick in the brain (S1). Students reported that debriefing sessions lead to reflection and knowledge development which could be put into clinical practice: These are real cases, and when we have to face it in our future work in (emergency services) or some other place, I’m sure that I will remember the simulation (S5). For male nursing students, undergoing maternity SimPs was an opportunity to access a ‘forbidden world’ and generate new knowledge: As everyone knows men are not allowed to apply for this job here [Qatar] in hospitals because of the (gender) roles. But still I should learn (S6) and I have learned many complications for postpartum and the most dangerous complication of what we have learned is haemorrhage. I have learned ways of breastfeeding and latch on to the baby(S6).
Educators considered it important to develop students’ identity as healthcare professionals: one educator stated [they] adapt to making someone else the priority, unlike at uni where everything revolves around them and their needs. On a normal placement the priority and focus are the clients, and the reality is that the students’ learning has to fit around (S7). Some educators used online video recordings and case studies to deliver virtual placements and felt that this method placed restrictions on the clinical decision-making process because We are coming to the clinical decision-making process (on the software) second-hand, ie following someone else’s thinking and the rationale is not necessarily provided (S6).
SPs and role-play with student peers offered an opportunity to develop communication skills. During SimPs, students realized that communication is not just about talking to the patient but also about looking and listening: You listen to what they say and not only the words but rather it was about spending time with them (S4). Students also understood the value of communicating with each other about roles and responsibilities before and during the patient encounter: We should also be quick in discussing what to do first and what to know first in order to gain time. Finally, we need to have a leader in the room to manage the work (S6).
Students avoided communicating with SPs when they didn’t know answers to the SPs questions. One student said, I think my strategy is to keep going despite the question. I’m not going to tell her, ‘Hold on, I’ll be back’, go check for the answer and come back. I would say whatever comes to me and keep on going (S6). Educators were able to encourage reflection on poor communication practices and impress upon students the importance of providing answers. Students also acknowledged their improved confidence in communication when they were able to provide information that was understood by simulated patients: I was giving the information well using simple information which could be understood by the mother (S6).
Finding 2 encompassed three categories: emotional response, facilitator’s role and collaboration with peers.
Most SimPs were undertaken as group activities and participants in most studies felt a range of emotions such as awkwardness, anxiety, fear of being exposed and embarrassment due to the newness of the experience. Anxiety was the most commonly recorded emotion, particularly with one student stating …at first, I felt a little lost, anxious, and scared because I did not know what to expect from simulation (S3). The thought of being judged by educators caused embarrassment and discomfort which in turn affected students’ performance: Even though you really mean to do something good… you end up doing something wrong anyway because you are so afraid [of what the teacher thinks] (S1). However, repeated exposure to simulation and tutor contact allowed students to overcome this negative effect: …but the relationship with tutors and the progression of simulation sessions, turned my embarrassment into comfort (S3).
Facilitators played an important role in motivating students and creating a positive or negative environment: 90% of it is the facilitator … on certain occasions [I] felt beat up (S5). A non-authoritarian style of facilitation contributed towards the students’ positive experience of simulation. Educator debriefing in identifying both mistakes and correct students’ action and instilling values appropriate for clinical practice compelled students to reflect upon their performance during the scenarios: I had the opportunity to review the appropriateness or not of my actions by means of both the directions given by the tutor and a better comprehension of theoretical rationale. These also contributed to the development of my critical thinking (S3).
Most SimPs were carried out in groups and collaboration with peers was integral to the placements. Educators observed that peers formed a social environment during SimPs in the absence of real patients and other healthcare personnel: Perhaps the group (or community) aspect of the simulated placement could be seen to replace or compensate for the lack of real or live players (S7). Students peer-reviewed each other’s performance though this received mixed opinions. Some educators felt this was an opportunity to give constructive feedback to each other ... such an important skill (S7). In contrast, some students felt that [When] the skills are assessed by our peers and if they’re not motivated, they just tick all the boxes (S4) without really being observant.
At times, working with peers was well received by students who felt that undertaking SimPs in groups helped them to develop professional skills and to feel comfortable to make mistakes: … since simulations were performed in groups of three, it contributed to my professional training, mainly as regards teamwork. Therefore, I professionally grew in defining leadership and roles with the ultimate aim of rescuing the patient’s life (S3). Sometimes group dynamics led to demotivation causing students to disengage from the learning experience: I really try to emotionally respond to the mannequin but sometimes in labs the other students just laugh at you and then you just don’t even try (S4).
Finding 3 encompasses three categories: perceived value, placement design and factors affecting implementation.
Students placed high value on the SimPs if they could link it to clinical practice which motivated them to immerse themselves in the learning experience: The main advantages are that students are trained, and their skills are refined to give a better result also in the operational field (S3). SimPs afforded students the opportunity of learning experiences they might never receive during clinical placements: There, I might only have the chance to do one newborn assessment but here I’m doing it more than once so I know what to do and I know what I’m not doing (S6). Educators acknowledged that traditional placement models do not allow students to undertake long-term follow-up with patients, which they can do in SimPs: to work through a case from the initial referral through to intervention is not an experience they would typically experience in their ‘real’ placements (S7).
Some students who came with high expectations were not disappointed: Personally, the expectations have not been betrayed and I felt improved from this activity (S3). For others, the increased value of SimPs was observed at completion of the placement, so much so that students recommended the continuation of SimPs in education: ... my expectations about simulations were not very high, I was also critic because I thought the laboratory was not provided with adequate equipment [...] I was very impressed with the laboratory and its realism (S3).
SimPs designed to deliver information in a concise manner was considered superior by students as it helped them to retain information without feeling overwhelmed: Tomorrow you will not remember a 200 page paragraph, but you will remember something concise, so you will say ‘I have to do this’ (S5). Students preferred being able to prepare in advance for simulation because this improved their performance which gave them a sense of reassurance: I think it is good if we knew the topics before the simulation sessions so we can prepare ourselves(S1). Role-play as clinicians created an active learning opportunity: So getting the chance to participate and taking the roles will give more knowledge and skills and it will last in their mind rather than only observing (S1). Students agreed that a greater number of simulation experiences helped strengthen learning and enhance their positive attitude towards SimPs: The organisation was excellent because gave us the opportunity to repeat simulation sessions for several times […] after having detected our mistakes, we tried to deal with them by acting with further details and attention (S3). SimPs that focussed on teaching rather than assessing students had a more profound impact on learning, as tension was replaced by curiosity: … we did not feel the tension from ‘we are going to be evaluated’; we entered the room with the intention of finding out ‘what is he going to give us?’ and see if we are able to do it (S5). Students suggested that when having to learn a new skill in a simulation scenario with mannequins I focus on clinical skills as it’s difficult to engage with the ‘patient’ (S4). Consequently, there is a need for varied scenarios to test a range of technical and non-technical skills.
Educators particularly appreciated the freedom to design scenarios where they could pause the simulation and provide instantaneous feedback to the students: it was useful to be able to respond quickly to a gap in their knowledge and then devise something specific to plug in that gap (S7). Educators designed placements with multiple opportunities to provide feedback: I had designed the whole placement experience around a range of feedback opportunities, my intention to make this a really rich feedback experience (S7). Learning was more profound when students designed simulation scenarios for themselves: ... when it is time for us to be in charge of performing the case, since we had to explain it to the other classmates so that they learned the same thing as us, we put more emphasis on searching for scientific evidence, about how it can become more complicated and how it cannot become more complicated, how to resolve it and until when (S5).
Success of a SimP is dependent upon students, educators, technical staff, the institutions and other stakeholders. Educators identified that low commitment and complacency in some faculty members impeded the smooth delivery of SimPs: ... I’ve had to cancel full sessions of days of maybe 20 or 30 students just because that secondary person [cancelled] (S2). Variation in the training of faculty created challenges: ... you sometimes are going to have people that have been trained with different levels of simulation experience before they get into the level that we’re at. So, we have to sort of bring everybody on to the same level (S2). Training and preparation of simulation facilitators were considered essential: education for faculty to understand simulation and how to make it happen is essential (S2).
Another barrier was the lack of approval from professional bodies towards substituting clinical hours with simulated hours despite the challenges of securing clinical placements: It’s hard to do a formative [simulation] when you don’t have buy-in from the credentialing body (S2). Educators agreed that support from stakeholders made it easier to conduct such placements: ... I think having the stakeholders with the commitment is really a positive way to get started (S2). Additionally, the expenses involved in implementing simulated placements were identified: I think that we need, obviously, the financial resources to expand this simulation (S2).
Educators faced challenges with student engagement during online SimPs. Potentially due to student resentment at feeling forced to engage with SimPs instead of clinical placements or possibly inexperience at engaging with online activities: the silence of a muted space in which people are not always able to even have their cameras on, was totally different in this situation than it had been in the months of online teaching preceding this. The dynamic conversation I was used to and hoped for in a clinical placement at times felt stilted, organised, and regimented (S7). Educators felt that implementing SimPs was demanding and left them exhausted at times: So when the students...are here for about three days, and ... getting 100 students through ... is exhausting for everybody, the students, and the faculty, and the staff (S2).
Despite the challenges, educators expressed passion for SimPs which kept them going: I think one major positive is having faculty that have a passion for it because they go above and beyond what’s expected (S2). That passion made educators resilient in the face of barriers and led to the generation of ideas to overcome them.
This review, investigating AHP and nursing student’s and educators’ experiences of SimPs within healthcare, identified 69 findings and 138 illustrations from eight studies that were pooled into nine categories to produce three low-quality synthesized findings. The findings were related to the reality, emotions and opportunities/challenges associated with SimPs.
This review identified that despite initial misgivings, SimPs were viewed as a way to develop skills, critical thinking, confidence, competence and communication prior to clinical practice or in specialized, hard-to-provide areas. Clinical placements are imperative for the successful preparation of registered healthcare practitioners [18,19]. They enable students to familiarize themselves with their healthcare role, develop clinical judgement, implement their classroom learning in real-life situations, as well as develop technical and non-technical skills [20]. Current evidence suggests that up to 25% of clinical placement hours can be effectively and safely replaced by SimPs [21,22]. Larue and colleagues reported that there was no difference in student competence between clinical placement and SimPs in nursing [21]. However, the quantity of substituted hours needs further investigation with greater pedagogical rationale regarding hours rather than study design restrictions [23]. This review supports the implementation of SimPs to address placement capacity challenges, whilst simultaneously supporting student’s development from novice to qualified practitioner.
This review found that the perceived success of SimPs depended on the concept of ‘realism’. Students felt a lack of empathy towards mannequins, which is in line with observations in Bearman et al.’s review investigating whether simulation might develop empathetic behaviours in healthcare students [23]. They also identified that role-play, where students play the role of a patient followed by SPs, was more effective in promoting empathy compared to mannequins, which evoked feelings of embarrassment and discomfort. A quasi-experimental study, investigating nursing students administering an intramuscular injection using an SP with a strap-on injectable device compared to using an injection mannequin, found that the students receiving SP training were significantly more patient centred [24].
Student’s perspectives deviated from practical reality in several important ways. First, students reported that lack of time prevented the provision of holistic care to the patients in the simulation scenario. While more time could be allocated for the simulation, providing optimum care in a stipulated time frame is a key clinical skill. Second, students wanted simulation scenarios beforehand, so that they could prepare, which is frequently incompatible with real clinical situations. It is recommended that where possible SimPs ought to reflect real patients either through the use of real patients, standardized patients, real case studies, role-play, although this needs to be balanced by the cost of doing so and appreciating that mannequins serve a purpose. In addition, it is recommended that the time to prepare for and complete a simulation be factored into the simulation scenario according to whether this is the first SimP or follows on from a previous placement.
In this review, students reported stressful feelings, discomfort, anxiety and embarrassment which transformed into positive emotions by the end of SimP. These responses could be due to the novelty of simulation [25]. Using simulation as a model of placement remains in its infancy and students’ perceptions of its value and their emotional responses need to be considered. This review suggests that repeated exposure to simulation helps reduce these negative emotions. However, Hardenburg et al. found that repeated exposure to simulation did not reduce physiological markers of stress, that is, heart rate [26]. Repeated exposure seems to affect psychomotor competence and confidence [27]. It is hypothesized by the authors that continual participation in simulated scenarios enhances competence, confidence, knowledge and clinical judgement. Students acknowledged that peers and educators played an important role in positively or negatively influencing their simulation experiences. It is recommended that educators promote a non-judgemental and safe atmosphere where discomfort and embarrassment are acknowledged, where students can be vulnerable, and where student competence, confidence, knowledge and clinical judgement can be developed.
In this review, the use of debriefing was valued as a means of plugging gaps in student knowledge and providing constructive feedback following the simulation scenario. A study examining hands-on alone simulation compared with hands-on plus debriefing simulation for nursing students found that debriefing dramatically and significantly improved knowledge of heart failure [28]. Feedback offered by facilitators during the simulation scenarios and the debriefing sessions allows students to meaningfully reflect on their clinical decision-making and its consequences [29]. Experience of undertaking a simulation scenario, followed by a period of reflection and thinking during the debriefing, may allow students to prepare for their next simulation scenario or clinical practice [30]. It is recommended that debriefing be a cornerstone of SimPs where educators provide students with time to review decisions, actions, communication, their ability to deal with the unexpected, discuss with others, learn and modify behaviour as a result [31]. Educators need to be trained and familiar with the concepts of debriefing.
Students and educators shared several factors considered to be important for successful SimPs including variety in delivery with a clear focus on technical and softer skills, ownership of the scenarios, the opportunity to view prior to exposure, repetition of scenarios and co-production of scenarios. They reported that using simulation as an assessment tool increased emotional discomfort, as opposed to using simulation as a learning tool whereby curiosity in learning was generated. A number of barriers to successful SimPs were identified including low commitment or complacency amongst educators, low levels of support from professional bodies, cost and poor student engagement, particularly during online SimPs. MacKinnon et al. [20], in their systematic review of student and educator experience of maternal–child simulation training, similarly found that lack of faculty support, funds, human resources and technological support were major barriers to the implementation of simulation. Based on these findings, it is recommended that stakeholder support be sought prior to implementing SimPs. Clear learning objectives, co-production of scenarios with students and time for debriefing, and further repetition would be good practice in SimPs across healthcare. Training and preparation of simulation facilitators are considered essential.
This review used a range of databases, JBI guidelines and PRISMA reporting standards to ensure the high quality of this review. The confidence in the results is limited due to the low dependability of the included studies. This review included English-language-only studies, which is a recognized limitation. There was only one study from Allied Health Professions, although it seems likely that the findings are transferable.
The findings of this study suggest that students had an overall positive experience. SimPs have the capacity to overcome cultural or other barriers to diverse placement provision for all. Simulated placement can substitute part or all of a clinical placement, with a recommendation of up to 25% of placement hours overall. Stakeholder and financial backing along with availability of support staff and a motivated faculty are necessary for the successful implementation of simulated placements.
The lack of guidelines for the implementation of simulated placements is a potential barrier to their implementation. It is suggested that governing bodies support the development of recommendations and guidelines on the implementation of simulated placement in health education.
Further, high-quality research is required to better understand the experiences and perceptions of allied health students and educators of SimPs. Further investigation of the views of educators would help to increase our understanding of facilitators and barriers to SimP implementation, and the intrinsic motivating factors and training needs of educators. In relation to SimP design, further exploration of the value that co-production adds to the student’s experience of simulated placements is warranted.
This review, investigating AHP/nursing student’s and educators’ experiences of SimPs, identified that, though initially apprehensive, students valued their SimP experiences. Important elements were scenarios related to real-world situations, use of human simulated patients rather than mannequins, a judgement-free environment focussing on learning rather than evaluation and multiple opportunities for feedback. The role of the facilitator was considered important. Educators found SimPs to be physically, emotionally and mentally demanding. Barriers to the successful execution of SimPs include lack of faculty training, limited funding and poor institutional support. Intrinsic motivation and passion of educators played a major role in overcoming these barriers.
Supplementary data are available at The International Journal of Healthcare Simulation online.
All authors contributed to review process and write up of the article.
This review was not funded.
None declared.
Compliant with Sheffield Hallam University ethics for Masters dissertation - literature review.
No conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
 Experiences of students and educators with simulated placements in allied health profession and nursing education: a qualitative systematic review
Experiences of students and educators with simulated placements in allied health profession and nursing education: a qualitative systematic review
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets