The International Journal of Healthcare Simulation has been rebranded as the Journal of Healthcare Simulation. Please visit https://www.johs.org.uk to view all articles and for article submissions.
The International Journal of Healthcare Simulation has been rebranded as the Journal of Healthcare Simulation. Please visit https://www.johs.org.uk to view all articles and for article submissions.

Doctors from minority ethnic (ME) backgrounds and International Medical Graduates (IMGs) in the UK describe barriers to receiving effective feedback, and feel they are negatively pre-judged, as highlighted by Chopra et al. [1]. This is unfair and likely contributes to the attainment gaps (with regards educational outcomes/career progression) that adversely affect these doctors.
This novel educational day targeting senior medical educators (with at least 5 years’ teaching experience) aimed to raise awareness of barriers to effective feedback conversations between doctors from different backgrounds and develop skills to overcome these in practice.
We used different modalities to illustrate a range of ‘real’ feedback scenarios between individuals from culturally diverse backgrounds, followed by facilitated discussions with the intent to reflectively develop allyship behaviours.
In keeping with best practice around simulation-based training, the pre-brief was designed to introduce concepts, but also importantly to create a safe, respectful place for discussion around some issues of a sensitive nature. An Ethics Board was consulted around reporting this novel initiative.
Introductory presentations from faculty outlined the experiences of IMGs as reported by Al-Haddad et al. [2], the impact poor feedback has, core concepts and approaches including Kim Scott’s ‘Radical candour’ [3] and Erin Meyer’s work on cultural intelligence [4]. These focused on differences in perceptions of hierarchy and feedback styles between different cultures, and how these can impact conversations. These are novel concepts within NHS systems for educators, with no currently easily accessible simulation-based training programmes addressing them.
Participants watched a pre-recorded simulated feedback session, performed by actors. We used a modified ‘shadow-box’ technique of simulation-based learning where several ‘chapters’ of a pre-filmed simulation scenario were actively observed by the participants followed by a facilitated de-brief to unpack observations from all perspectives in the simulated case, also described by Mutch et al. [5].
Participants enacted two role-play feedback scenarios in pairs, followed by reflective discussion.
A live ‘immersive’ simulation was presented, where a professional actor (playing an IMG training doctor) role-played a scenario in front of the group with a faculty member playing the role of a supervisor. The group reflected on how the feedback conversation could be improved. One participant volunteered to role-play the supervisor and endeavoured to incorporate points from the discussion into the feedback conversation. The de-brief and reflections focused on the differences in the simulated versions and the contrasting responses elicited from the IMG training doctor/actor.
Learners moved across the various learning modalities during the day (Figure 1). In line with scaffolding learning theory, learners built upon their knowledge, developed skills, to then finally consider performance.

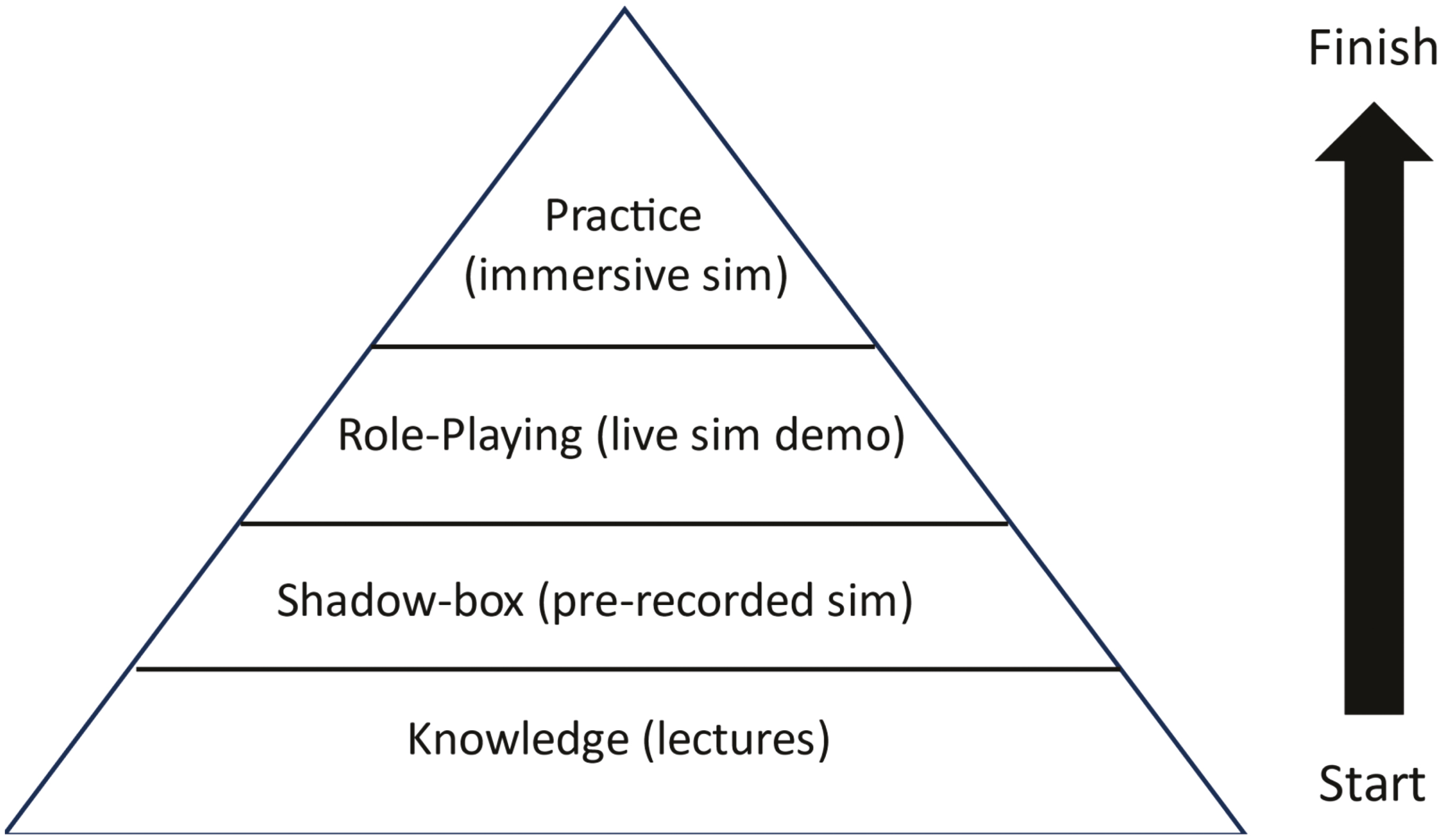
‘Fairer Feedback’ training day structure.
On the day, all 18 participants completed a printed evaluation questionnaire; their responses to 20 closed items are shown in Figure 2a and b.
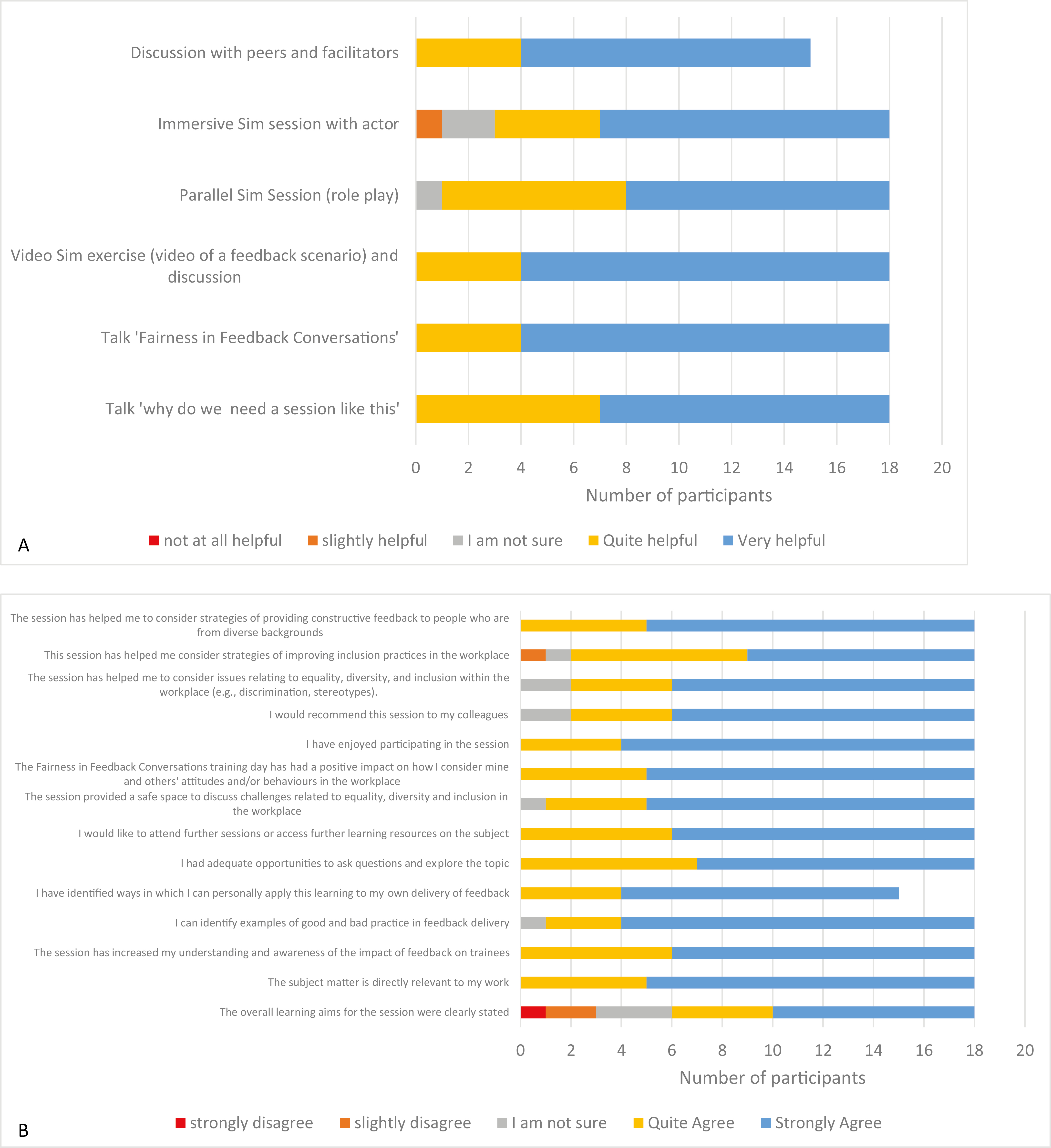
(a, b) Evaluation questionnaire responses.
The pre-recorded simulation scenario was perceived to be realistic and generated rich discussion around less than full-time training; impact of perceived biases in conversations with those from ME backgrounds (in this case a female, pregnant training doctor who wore a headscarf). Reflections included: missed opportunities to investigate difficulties that the doctor was experiencing; lack of clarity in setting objectives for the meeting; insensitivity and prejudice with regards to the training doctor’s position as an expecting mother. Other themes explored in this scenario included the impact of social exclusion in the workplace, the impact of micro-aggressions upon a doctor’s confidence and the effects of intersectionality.
The role-play scenarios included themes around Ramadan, religious sensitivity and addressing health concerns raised by an ME doctor.
Whilst role-play and video-based scenario discussions provided a non-threatening space for learners to explore ideas around cultural barriers to effective feedback conversations, the live immersive simulation provided an opportunity for learners to practice their feedback skills as well as ‘think on their feet’. The themes that emerged from the live immersive simulation session were around being alert and sensitive to the unique challenges related to migration (e.g. transport, childcare set-ups, financial challenges as well as acclimatising to a wholly different working culture).
Whilst experienced educators are well versed in providing support for doctors encountering difficulties (framed aptly by Maslow’s Hierarchy), a depiction of some of the unique challenges that affect IMGs was demonstrated by these simulated scenarios.
The ‘Fairer Feedback Conversations’ training day used multimodal simulation-based training to develop supervisors’ skills in conducting effective feedback conversations with doctors from diverse backgrounds.
Simulation-based training methods in developing non-technical skills are being increasingly utilized, particularly to develop team working, leadership and communication skills. Although there are themes emerging around how learners can generally engage with issues around diversity and inclusivity within existing simulation-based learning sessions, there is little evidence around how these training methods can be used specifically to develop inclusive behaviours that challenge implicit biases in the workplace. We aimed to contribute to the evidence on the use of simulation modalities for these purposes.
This training day provided educators with new knowledge and insights into ‘playing out’ feedback conversations with those from diverse backgrounds. By gaining such insights and opening up the challenging and sometimes uncomfortable discussions around the real, practical day-to-day implications of bias/stereotype/assumptions, we can start to genuinely promote equity and inclusivity in medical education.
None declared.
None declared.
None declared.
None declared.
None declared.
1.
2.
3.
4.
5.
 Fairer feedback – enhancing feedback conversations between those from diverse backgrounds
Fairer feedback – enhancing feedback conversations between those from diverse backgrounds
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets