
Understanding team behaviours leading to successful outcomes in resuscitation could help guide future training. Guidelines recommend defibrillation for shockable rhythm cardiac arrests within 2 minutes. This observational pilot study aimed to determine whether teamwork behaviours among medical trainees differed when time to defibrillation (TTD) was less than 2 minutes, versus 2 minutes or more.
Following ethical approval, groups of six internal medicine trainee (IMT) doctors in Scotland formed an ad hoc team in high-fidelity immersive simulation (shockable rhythm cardiac arrest). TTD was recorded. Video-recordings were scored by two researchers independently using the Team Emergency Assessment Measure (TEAM) tool. Differences between TEAM scores in the fast TTD versus slow TTD groups were compared using Student’s t-test.
Twenty-three videos involving 138 trainees were scored using the TEAM tool. Scores ranged from 19–39.5/44 (mean 28.2). Mean TTD was 86.2 seconds (range 24–224), with 17/23 teams achieving defibrillation in under 2 minutes. Those achieving fast TTD achieved higher TEAM scores, and the result was statistically significant (30.1 ± 5.0 vs 22.9 ± 3.3, p = 0.004). When analysing the statistical significance of the differences in individual TEAM items, there was a statistically significant difference in the fast TTD and slow TTD groups for item 7 (adaptability).
This observational pilot study found that improved team performance, as measured by the TEAM tool, was associated with faster defibrillation by IMT doctors in simulated cardiac arrest. It highlighted the importance of adaptability as a team behaviour associated with successful performance, which is of interest to those involved in training high stakes emergency teams.
What this study adds
Non-technical skills (NTS), also referred to as behavioural skills [1,2], play a crucial role in cardiac arrest resuscitation performance, both in the simulated and clinical environments [3]. Poor performance in NTS has been highlighted in resuscitation teams [4] and it is recognized that team dynamics can influence the efficiency of clinical tasks being performed in resuscitation [5]. Due to positive impact on patient outcomes, an inpatient rapid response team or medical emergency team (MET) will respond to calls signalled due to patient deterioration or cardiac arrest in most hospitals [6,7]. In the United Kingdom (UK), the MET will usually comprise of a combination of medical and nursing staff and is an ad hoc team, the members of which may vary on a day-to-day basis. However, outcomes from cardiac arrest remain suboptimal and ensuring effective training interventions is key to enhancing patient safety [8,9]. There is evidence that team training can lead to improved patient outcomes [10–12] and that immersive simulation can be utilized in this context [13,14], which can build social capital for ad hoc teams [15].
Although NTS are recognized as important in improving team performance, further assessment is required to delineate more specifically which team behaviours are key to optimal performance. NTS are defined as the cognitive and interpersonal skills, such as leadership and teamwork, that contribute to efficient team performance [16]. There have been calls to use the term behavioural skills [2], defining them in a positive sense rather than ‘non-technical’ which could be seen as subordinate despite their importance [1]. Immersive simulation can provide a valuable modality and opportunity for research into such behaviours [17]. For example, previous research has used discourse analysis to examine team talk in medical emergencies, exposing communication strategies used to create shared team situational awareness [18,19]. Behavioural marker systems or NTS assessment surveys are tools that can measure teamwork and provide insight into behaviours that lead to successful performance [20]. Observing and understanding behaviour is enlightening but we must strive to better understand the specific team behaviours that can lead to successful, or unsuccessful, outcomes. Immersive simulation can provide an authentic environment to observe team behaviours to advance our understanding of teams in these contexts, and the specific aspects resulting in optimal performance in an objective manner. Absence of leadership can lead to unsuccessful outcomes [14,21]; however, it has been recommended that better understanding of the influence of specific team behaviours and team dynamics in such situations would be beneficial to guide training efforts [14,22,23].
Improving understanding of the importance of specific team behaviours in the setting of cardiac arrest could guide feedback provided in the debriefing session following simulated scenarios and aid medical educators more widely to focus on key areas. To investigate this and provide practically helpful information to trainers, defining the outcome of a successful team performance is key. Resuscitation guidelines recommend defibrillation as early as possible for shockable rhythm cardiac arrests [6], with improved outcomes when defibrillation is within 2 minutes [24,25]. Therefore, in the context of cardiac arrest with a shockable rhythm, one way of defining successful team performance is delivery of a shock within 2 minutes of arrest [24,25]. In the UK, the MET often includes internal medicine trainees who, as they progress through their training, will step into the role of team lead for resuscitation teams. It is recognized that junior doctors require training in NTS for managing emergency situations [26]. Better understanding their team behaviours leading to successful performance could inform such training strategies.
The aim of this pilot study was to determine whether teamwork behaviours among internal medical trainees differed when time to defibrillation (TTD) was less than 2 minutes, versus 2 minutes or more.
This study received ethical approval from the NHS Education for Scotland ethics review board, reference number NES/Res/14/20/Med. All participants gave informed written consent for data collection and the publication of anonymized results. Participants were free to leave the study at any time without giving a reason.
Internal Medicine Training (IMT) is a 3-year training programme for junior doctors in the UK who wish to pursue a career in medical specialties. In Scotland, simulation-based education is integrated into each year of the training programme, including a 3-day IMT boot camp within the first year. The IMT boot camp incorporates immersive simulation in addition to communication workshops and simulation-based mastery learning of procedural skills. It is recognized that teamwork and leadership training can improve resuscitation outcomes [14] and, as such, simulation-based training aims to develop IMT doctors’ NTS in leading cardiac arrest teams. The high-fidelity immersive simulation involves six acute care scenarios spread over 3 days. Between August 2020 and January 2022, the IMT boot camp was delivered to 230 IMT doctors at the Scottish Centre for Simulation and Clinical Human Factors (SCSChf) in Larbert.
Trainees were orientated to the simulation environment and mannequin at the start of the course, including equipment such as the defibrillator. The simulated environment consisted of a single, full-body adult mannequin simulator (SimMan Essential; Laerdal) accompanied by paperwork, monitoring equipment and adult resuscitation trolley. Three ceiling-mounted cameras allowed each scenario to be filmed from a variety of perspectives. The patient voice was transmitted via a wireless microphone and a bedside monitor displayed dynamic physiological parameters. A member of simulation centre staff played the role of a nurse within each scenario. Each 15-minute scenario was followed by a debriefing session led by boot camp faculty members.
IMT doctors participated in groups of six as an ad hoc team with one trainee taking the lead in each scenario, entering the simulation environment on their own initially with the opportunity to call for help. Prior to entering the simulation environment, the trainees were given a brief from a faculty member that a member of nursing staff had asked for review of a patient with either chest pain, agitation or palpitations. One trainee entered the scenario first and the other trainees entered when the initial participant called for help or a cardiac arrest call. The scenario used in this study involved a patient who has been admitted with ventricular tachycardia with a pulse, who required direct current cardioversion due to adverse features of shock. The patient subsequently deteriorated into ventricular fibrillation. All group participants were involved as the cardiac arrest team, with the original ‘hot seat’ participant expected to act as team leader, unless otherwise agreed by the team. Return of spontaneous circulation occurred following successful defibrillation with a second unsynchronized shock.
Video-recordings of the scenarios in which all participants had provided written consent for observational study were saved. To assess the team behaviours the videos were observed by two researchers independently and team behaviours were scored using the validated Team Emergency Assessment Measure (TEAM) tool [27]. The use of a behavioural marker system allows a more objective assessment of specific observed behaviours to address the research question [28]. The TEAM tool was chosen as it is well-recognized, was designed for emergency teams and has been validated in similar contexts [29–35]. The TEAM tool consists of 11 items scored on a 0 to 4 (never to always) scale and an overall global assessment score on a 1 to 10 scale with 1 = poor and 10 = excellent. The TEAM tool covers three categories of NTS performance; leadership (two items); teamwork (seven items); and task management (two items).
In April 2021, the research team registered for the TEAM brochure which provides guidance for use of the TEAM tool for raters. Both raters were experienced clinicians with faculty roles within simulation-based education and experience of managing medical emergencies. The TEAM brochure includes a rating matrix with example behaviours for low and high scores which was utilized by raters. Time from cardiac arrest to first defibrillation (TTD) was recorded in real time for each scenario by simulation faculty.
No prior data were available to perform a sample size calculation, and this study was therefore considered a pilot. The mean scores of the two raters were used for analysis. We aimed to test for normality using the Kolmogorov–Smirnov test. We would compare differences between the overall TEAM scores and the individual TEAM items in the fast (<2 minutes) TTD versus slow (2 minutes or more) TTD groups using Student’s t-test (if the data were parametric) or the Mann–Whitney U test (if the data were non-parametric). We considered the difference to be statistically significant if p < 0.00417 (5% significance level with Bonferroni correction for multiple comparisons). Statistical analyses were performed using IBM SPSS Statistics version 28.0.1.1.
Twenty-three videos involving 138 trainees were reviewed, including doctors from all four Scottish training regions. TEAM scores ranged from 19–39.5 (mean 28.2) out of a possible 44 and leadership scores ranged from 1.5–7.5/8 (mean 4.4). Mean TTD was 86.2 seconds (range 24–224 seconds), with 17/23 teams achieving defibrillation in under 2 minutes.
The Kolmogorov–Smirnov test showed that the data were normally distributed, and therefore we used Student’s t-test to compare difference between means. Those achieving fast TTD achieved higher TEAM scores than those achieving a slow TTD, and the result was statistically significant (30.1 ± 5.0 vs 22.9 ± 3.3, p = 0.004). This is shown below in Figure 1.


Means and 95% confidence intervals for TEAM scores in the fast versus slow time-to-defibrillation groups.
Those achieving fast TTD achieved higher mean scores in every TEAM item, as shown in Figure 2.
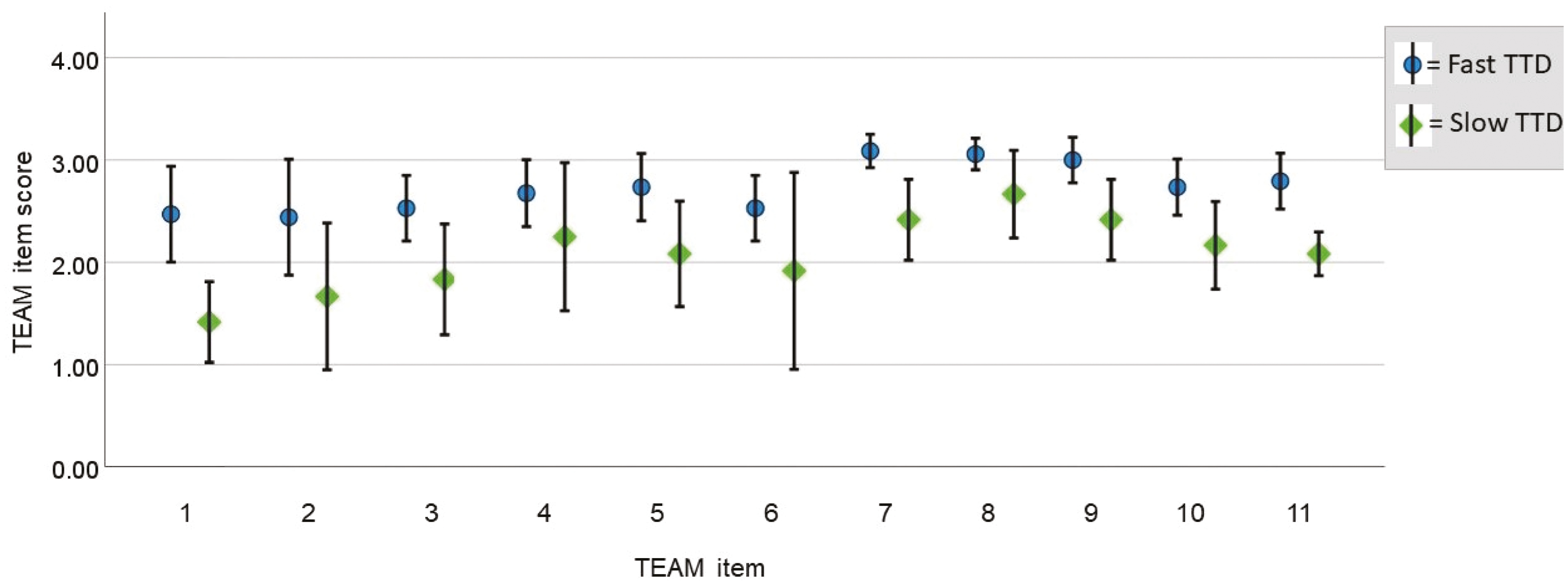
Means and 95% confidence intervals for individual TEAM item scores for the fast versus slow time-to-defibrillation groups.
When analysing the statistical significance of the differences in these means, only one of the differences is significant at the 5% level (with the Bonferroni correction). This is item 7 – ‘the team adapted to changing situations’ (see Table 1).

| TEAM item | Fast TTD group Mean (SD) |
Slow TTD group Mean (SD) |
p-value |
|---|---|---|---|
| 1. The team leader let the team know what was expected of them through direction and command | 2.47 (0.91) | 1.41 (0.38) | 0.01272 |
| 2. The team leader maintained a global perspective | 2.44 (1.10) | 1.67 (0.68) | 0.12414 |
| 3. The team communicated effectively | 2.53 (0.62) | 1.83 (0.52) | 0.02355 |
| 4. The team worked together to complete the tasks in a timely manner | 2.68 (0.64) | 2.25 (0.69) | 0.18096 |
| 5. The team acted with composure and control | 2.74 (0.64) | 2.08 (0.49) | 0.03475 |
| 6. The team morale was positive | 2.53 (0.62) | 1.92 (0.92 | 0.08152 |
| 7. The team adapted to changing situations | 3.09 (0.32) | 2.42 (0.38) | 0.00036 |
| 8. The team monitored and reassessed the situation | 3.06 (0.30) | 2.67 (0.41) | 0.02036 |
| 9. The team anticipated potential actions | 3.00 (0.43) | 2.42 (0.38) | 0.00812 |
| 10. The team prioritized tasks | 2.74 (0.53) | 2.17 (0.41) | 0.02782 |
| 11. The team followed approved standards and guidelines | 2.79 (0.53) | 2.08 (0.20) | 0.00482 |
This observational pilot study assessed the team behaviours of IMT doctors in simulated cardiac arrest scenarios using the TEAM tool and measuring the TTD. The analysis shows that higher TEAM scores are associated with a faster TTD. When analysing individual TEAM score items, there was a statistically significant difference between the fast TTD and slow TTD groups in the skill element of adaptability.
Although the majority of teams (17 out of 23) achieved defibrillation within 2 minutes, there is evidence of significant delays in defibrillation in studies exploring real clinical practice [24,36]. Given that higher TEAM scores were associated with a faster TTD in this cohort, this suggests we should strive to improve TEAM scores where possible [14]. Utilization of the TEAM tool as part of IMT simulation training could be considered to try to achieve this by providing formative assessment and tangible suggestions for improvement.
From our analysis, fast TTD and slow TTD groups showed a statistically significant difference in item 7 within the team work category, ‘the team adapted to changing situations’. This suggests that adaptability is a key team behaviour required for successful performance. It is a recognized core component of teamwork defined as the ‘ability to adjust strategies based on information gathered from the environment’ leading to an altered course of action in response to changing conditions [37]. It is through breaking down the components of teamwork that we will develop a clearer understanding of what constitutes good teamwork and how best to provide training for successful performance [37]. Adaptability must be maintained in emergency situations [38] and is reliant on shared mental models and performance monitoring leading to coordinated action [37]. Adaptive coordination has been shown to be important in performance in anaesthesia in moving from implicit to explicit coordination whereby explicit coordination statements are expressed in an unambiguous manner with the intent to coordinate behaviour [39–41]. This would apply in the scenario of this study with the recognition of cardiac arrest as a cue which prompts a shift to the cardiac arrest algorithm and coordination of early defibrillation [42]. The importance of cue recognition and this shift could be a focus for training and a key learning point during the simulation debriefing session, particularly if there has been a delay to defibrillation due to a lack of adaptability. Adaptive behaviours have also been included in a taxonomy from a recent scoping review of the NTS required by ad hoc teams, suggesting teams with a strong team mental model with regular situation updates will have improved adaptability, another potential focus for training for success [43]. Considering adaptability and the related concepts such as cue recognition and explicit coordination are important in helping learners understand what adaptability in teamwork means and what we should be striving towards in practical terms [44].
This observational pilot study assessed the team behaviours of a national sample of IMT doctors. The use of immersive simulation provided consistency within the scenario. It is recognized that the scenario involves IMT doctors and nurse confederates but, in real clinical practice, the grade of doctors attending cardiac arrests would be more varied. The raters lacked experience of using the TEAM tool prior to the study; however, they were experienced in the use of similar behavioural marker systems and were well versed from the training brochure prior to the study period. It was not possible to completely blind the researchers to the TTD as they were watching the videos; however, the researchers were motivated to focus on the team behaviours, and had a genuine desire to find out whether team behaviours were related to TTD, and therefore had no reason to artificially inflate scores in the fast TTD group. In addition, the trainees were not aware of the specific recording of TTD, which should have prevented them altering their behaviour to achieve this.
Further work could focus on the specific team behaviours that are associated with reduced TTD. This could be achieved with larger participant numbers and a regression analysis to assess the biggest impact on TTD. This study adds merit to the aims of the IMT simulation strategy in improving teamworking and leadership skills in these situations. The utilization of the TEAM tool with trainees to aid reflection on performance and provide focus for areas of improvement could be considered.
This observational pilot study found that improved team performance, as measured by the TEAM tool, was associated with faster defibrillation in simulated cardiac arrest for IMT doctors. It highlighted the importance of adaptability as a team behaviour associated with successful performance, which is of interest to those involved in training high stakes emergency teams.
The authors thank all of the trainee participants and Julie Mardon and Tanya Somerville for their support and provision of access to the Scottish Centre for Simulation and Clinical Human Factors for this research.
JK led the conception and the design of the study, data collection, analysis and interpretation of the data, and the drafting and the revision of the manuscript. RK contributed to the conception and design of the study, data collection and the drafting and the revision of the paper. SES contributed to the conception and design of the study, the analysis and interpretation of the data, and the drafting and the revision of the paper. VRT contributed to the conception and design of the study, the interpretation of the data, and the drafting and the revision of the paper. All authors (JK, RK, SES and VRT) approved the final manuscript for publication and have agreed to be accountable for all aspects of the work.
This study was supported through the IMT Simulation Strategy via NHS education for Scotland.
None.
This study received ethical approval from the NHS Education for Scotland ethics review board, reference number NES/Res/14/20/Med.
The authors declare no conflict of interest.
Data available from authors upon reasonable request.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
 Assessing team behaviours and time to defibrillation during simulated cardiac arrest: a pilot study of internal medicine trainees
Assessing team behaviours and time to defibrillation during simulated cardiac arrest: a pilot study of internal medicine trainees
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets