Corresponding author: Cathy M Smith, [email protected]
” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-cathymsmith”>Cathy M Smith, 2 Faculty of Health Sciences and Medicine, Bond University, Gold Coast, Australia3 Department of Emergency Medicine, Gold Coast Hospital and Health Service, Gold Coast, Australia
” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-nematalsaba”>Nemat Alsaba, 4 School of Clinical Sciences, Faculty of Medicine, Nursing & Health Sciences, Monash University, Clayton, Australia5 Department of Surgery, University of Melbourne, Melbourne, Australia
” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-debranestel”>Debra Nestel, 6 Health and Community Studies, Sheridan College, Toronto, Canada7 Speech Pathology, University of Toronto, Toronto, Canada
” class=”pop” data-container=”body” data-toggle=”popover” data-placement=”bottom” href=”../../../search_author-lisasokoloff”>Lisa Sokoloff
Simulated participants (SPs) can support development of competencies associated with person-centred care of older adults. There is limited information and understanding about working with older adult SPs and those who support them to create authentic, safe and effective simulations. This review aimed to review simulation literature focused on the care of older adults to explore and summarize what is known about working with older adults as SPs in healthcare providers’ education.
This scoping review followed Arksey and O’Malley’s five-stage approach, involving identification, selection, charting, collating, summarizing and reporting on results. Databases searched included MEDLINE, PsychINFO and EBSCO. To capture additional articles, we hand-searched the reference lists of articles selected for inclusion, MedEdPORTAL and Google Scholar.
From the initial 816 citations identified, 12 articles were in scope. Articles were either research or educational guides. Findings related to general characteristics of articles, description of SPs, conceptualization of SP role/scenario, SP preparation and scenario implementation.
Older adult SPs contribute to healthcare provider training in authentic, engaging, safe and effective ways. This scoping review provides a foundation on which to further develop older adult SP practices by highlighting their well-being and safety (both physical and psychological), promoting ways to increase diversity and inclusion, and emphasizing that the words we use matter. Improved reporting details of articles involving older adult SPs will facilitate the identification of effective practices.
What this study adds
Globally our population is ageing. Older adults are identified by the United Nations (UN) and World Health Organization (WHO) as individuals as being 60 years and older [1,2]. By 2050 the number of older adults is projected to reach 2.1 billion [2]. The care of older adults is challenging due to complex multidimensional medical, psychosocial and physiological age-related changes [3]. Upskilling and training of future healthcare providers and caregivers are required to improve older adults’ care and health outcomes [4].
Simulation focused on the care of older adults, also referred to as geriatric simulation, is an educational method that can be integrated into healthcare systems and training programs to improve the care of older adults by enhancing healthcare provider education and promoting the application of skills learned in simulation into practice [3]. Designing and delivering this kind of simulation encompasses specific considerations, including selecting an appropriate simulation modality. Simulated participants (SPs), a term first articulated by Bearman and Nestel [5] and later adopted by the Association of SP Educators in their Standards of Best Practice [6], is an inclusive term for any human role player in simulation. SPs are well people carefully trained to portray others such as patients, family members or clients for educational, assessment and research purposes. SPs can support development of competencies associated with person-centred care of older adults [7]. Eklind et al. note that ‘… person-centered care broadens and extends the perspective of patient-centered care by considering the whole life of the patient’ ([8] p10) rather than just their experience as a patient.
There has been a progressive and exponential increase over the past decades of interest in and reporting on simulation for the care of older adults. To get a broad sense of the growth of interest in the topic, we conducted a Google Scholar search (28 November 2022) using the terms ‘Geriatric simulation’ OR ‘Gerontological simulation’. The search yielded the following results: 3,400 (1990–1999); 11,300 (2000–2009); 17,600 (2010–2019); and 11,500 (2020–2022). Articles appear to focus on learner outcomes, training for educators/healthcare providers/simulationists, and program objectives while few focus on older adults as SPs. If SPs are involved or mentioned there is generally minimal information provided about them or how they are supported in their work. Further, in some of these activities, older adults are reported as being portrayed by much younger adults, which may run the risk of stereotyping and promoting ageism.
There are standards of practice for working with SPs that provide five underlying Values (safety, quality, professionalism, accountability, collaboration) and five Domains (safe work environment, case development, training SPs, program management, professional development) [6]. However, these standards do not consider nuances related to age (e.g. children, adolescents) [9]. Specific considerations for working with older adult SPs have been developed, relating to physical, cognitive and sensory changes that older adult SPs may experience [7]. However, there is limited information and a lack of broader understanding about working with older adult SPs and those who support them to create authentic, safe and effective simulations. We chose a scoping review methodology because we were seeking to explore this topic broadly and wanted to allow for the possible inclusion of many different types of articles [10].
The aim of this study was to review the simulation literature related to the care of older adults in order to explore and summarize what is known about working with older adults as SPs in healthcare providers’ education.
The authors have significant experience in healthcare simulation practice, with diverse roles as educators, healthcare providers and researchers. Our backgrounds include emergency medicine with a special interest in the care of older persons (NA), medical speech-language pathology (LS), education (DN) and performance (CS). We all have extensive experience working with SPs and with older adult SPs in several countries, including Australia, Canada, Hong Kong and the United Kingdom. We came together to undertake this scoping review due to a shared curiosity around this topic. Individual experiences informed discussion at each stage of the scoping review process, which proved valuable, especially in checking assumptions.
This review was guided by the five-stage approach described by Arksey and O’Malley [10]. We chose to follow this framework as the seminal method in scoping review methods.
While our broad topic was simulation related to the care of older adults, we wanted to identify what was known about older adults working as SPs. We had a specific interest in the nature of older SP involvement, their training and approaches used to study their practices. We framed the research question broadly as: What is known about older adults working as SPs in healthcare providers’ education?
To answer the research question, specific criteria were set regarding which articles to include in the review. The search focused on articles that addressed simulation activities involving older adult SPs. Only articles written in English and published between 2011 and 2021 were included. We chose 2011 as the start date as we wanted to capture articles that were relevant to more current practices. We excluded articles written in languages other than English as we did not have the resources (time, money) to have them translated in a reliable manner. We developed and refined an iterative search strategy in consultation with academic librarians experienced with healthcare databases (see Table 1 for a list of these search terms). In keeping with the open-ended research question, we sought to include a broad range of perspectives, including research, commentaries, essays and simulation scenarios. In keeping with this type of scoping review, we did not assess the quality of the research [10]. Our search had three phases. First, we accessed the MEDLINE database (December 2021), and then two additional databases: PsychINFO and EBSCO (February 2022). To capture any additional articles, we hand-searched the reference lists of articles selected for inclusion as well as MedEdPORTAL. We also searched Google Scholar (June 2022) with a modified list of search terms (see Table 1 for the list of these search terms). Additional articles were generated through this search. Citations were imported to Covidence Systematic Review Software (Melbourne, Australia).

| Database searched | Search terms used |
|---|---|
| MEDLINE PsychINFO EBSCO |
Group 1 Patient simulation OR Simulated patient OR Standardized patient OR Simulated participant OR Programmed patient OR Actor OR Role-player OR Confederate AND Group 2 Aged OR Geriatric OR Older OR Senior OR Elderly AND Group 3 Simulation AND Group 4 Dementia OR Stroke OR Falls OR Elder abuse OR End of life |
| Google Scholar | ‘Simulated patient’ OR ‘Standardized patient’ OR ‘Simulated participant’ OR ‘Actor’ AND ‘Older adult’ OR ‘Senior’ OR ‘Elderly adult’ AND ‘Simulation’ OR ‘Geriatric simulation’ or ‘gerontological simulation’ or ‘simulation for the care of older adults’. |
All abstracts were screened by the four researchers in teams of two (variously configured). Full-text reviews were similarly undertaken. Inclusion criteria were refined through this process. Articles had to mention involvement of older adult SPs, although various terms could be used to refer to them other than SP (e.g. actor, volunteer). In line with the UN and WHO definition of an older adult, we required specific reference in the article to SPs being at least 60 years old. Articles where the SP age was described as ‘older’, ‘elderly’ or as having an age similar to that of the older adult being portrayed in a scenario were also included. The exclusion criteria were set by consensus of all authors (Table 2). Articles describing the involvement of SPs under the age of 60 portraying older adults (e.g. a younger person portraying the role of an older adult) were excluded as we were focusing on the practices of older SPs. During this process, conflicts were discussed, and consensus was achieved during regularly scheduled meetings between authors.
| Article written outside of timeline for search |
| Simulation is focused on older adults, but the age of the SP is not clear |
| Simulation is not focused on older adults or SPs |
| Not clear if older SPs were involved |
| Minimal description of involvement of older SPs |
| Simulation involved a younger person (e.g. student) portraying a person 60 years or older |
| Simulation used a mannikin rather than human SP |
| Simulation has a person (e.g. family member, health professional) who is younger than 60 and no human role player 60 or older |
| Simulation involves a person 60 or older with actual findings who is recruited to work with students and is not trained in SP methodology |
We then charted the data. Charting refers to the process of obtaining key items of information from the included articles [10]. We created a template in Covidence with headings containing these key items. We piloted the template by independently applying it to one article, meeting to discuss, addressing any disagreements, coming to consensus and further revising any items that had not been clearly interpreted by the group. We repeated this process in pairs with a second article. At this point, we considered our group understanding to be calibrated, so we evenly divided the remaining articles between authors to independently complete extraction to Microsoft Excel (Microsoft, Redmond, USA). Extracted data included general characteristics about the article (e.g. year of publication, country of first author, type of journal, type of article, type of research), description of SPs (e.g. terms used, reported age), conceptualization of SP role/scenario (e.g. terms used to describe role, format of role, information provided in role, scenario details, development of SP role/scenario), SP preparation (e.g. recruitment, training for role portrayal, training for feedback and debriefing with learners) and scenario implementation. All authors reviewed the extracted data for accuracy, both individually and as a group where initial impressions were shared. Each author then did a deeper analysis of assigned sections of the data. The authors collaboratively discussed their analysis and addressed any disagreements to achieve consensus.
The analysis of key characteristics of the data was summarized and reported in the results below.
From the initial 816 citations, 74 duplicates were removed, leaving 742 abstracts to be screened. Through the title and abstract review, 614 articles were deemed out of scope. A full-text review was completed on the remaining 128 articles. Articles without abstracts progressed to full-text review. A further 116 articles were excluded. The main reason for exclusion was that the simulation was not focused on older adult SPs. Many articles either did not report the age of the SP or did not clarify if or how older SPs were involved. Twelve articles [11–22] were deemed in scope (Figure 1; Table 3).
| First author | Citation | Year | Title | Journal/publication |
|---|---|---|---|---|
| Baylor, C | [11] | 2017 | Assessing the believability of standardized patients trained to portray communication disorders | American Journal of Speech-Language Pathology |
| Davis, K | [12] | 2017 | Utilizing older adult standardized patients to enhance the education of health professional students | Case Studies from Age in Action |
| Dugmore, H | [13] | 2020 | Interpreting the value of feedback: older adult feedback to nursing students in a simulated environment in residential aged care | Nurse Education in Practice |
| Karnish, K | [14] | 2019 | Interprofessional socialization through acute-care simulation | Radiologic Technology |
| Lee, DA | [15] | 2021 | “This Is Me!” Perceptions of older adult simulated participants in an aging and injury simulation experience | Journal of Trauma Nursing |
| Quail, M | [16] | 2016 | Student self-reported communication skills, knowledge and confidence across standardised patient, virtual and traditional clinical learning environments | BMC Medical Education |
| Sarzynski, E | [17] | 2014 | An OSCE to assess trainee management of complex older adults and to teach documentation, coding, and billing | MedEdPORTAL |
| Schelgel, C | [18] | 2019 | “Please let me know when I do not realize it myself”: a qualitative analysis of senior simulated patients’ experiences | Advances in Simulation |
| Shawler, C | [19] | 2011 | Palliative and end-of-life care: using a standardized patient family for gerontological nurse practitioner students | Nursing Education Perspectives |
| Smith, CM | [20] | 2021 | “It’s like a shot in the arm”: evaluating the experiences of older simulated participants in structured virtual meetings during COVID-19 | International Journal of Healthcare Simulation |
| Soong, AD | [21] | 2011 | Interviewing a grandparent caregiver with age-related hearing loss | MedEdPORTAL |
| Thompson, J | [22] | 2017 | Older people’s views and experiences of engagement in standardised patient simulation | BMJ Simulation & Technology Enhanced Learning |

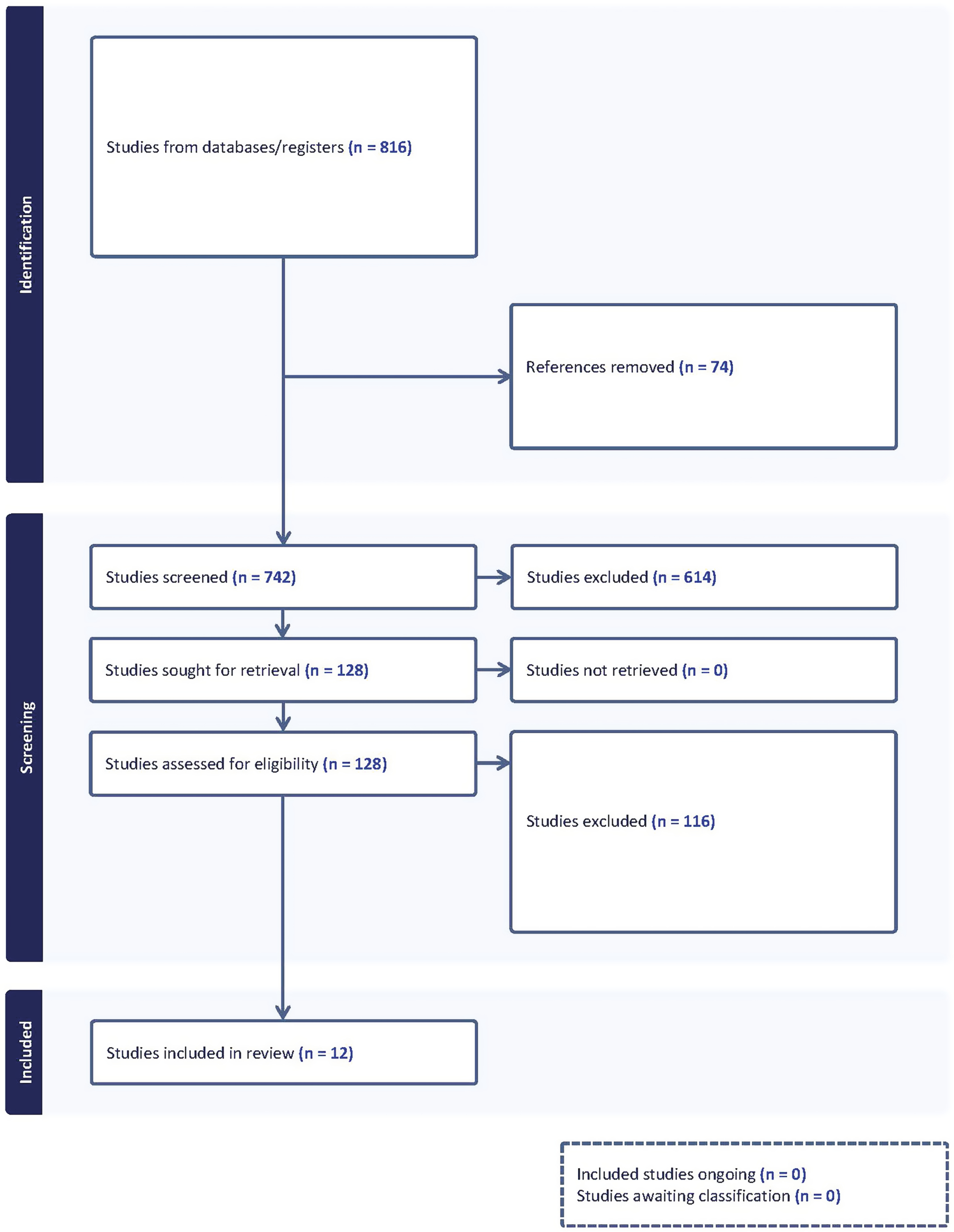
Prisma flow diagram.
More articles were published in the latter half of the decade, 2017–2021 [11–15,18,20,22] than between 2011–2016 [16,17,19,21]. Based on the first author’s place of work, all articles were from the Global North. The majority of articles were generated from the United States [11,12,14,15,17,19,21], with two from Australia [13,16], and one each from Canada [20], Switzerland [18] and the United Kingdom [22]. Journals had an education [12,14,16,17,19,21], simulation [15,18,20,22] or profession-specific focus [11]; one journal focused on both education and profession [13].
Ten articles described older adult SP involvement in simulation scenarios [11–17,19,21,22]. Learners included specific student groups [12–14,16,21,22], including an interprofessional group [14], and single healthcare professions [15,17,19,21]. One article did not mention the learner group [11]. The remaining two articles focused on SPs rather than learners [18,20].
Eight articles were research-based: five of these were qualitative [13,15,18,20,22], and three were mixed methods [11,14,16]. Two research articles focused on learner outcomes [14,16], four explored SP methodology related to a specific simulation activity and/or the lived experiences of SPs [15,18,20,22], one focused on the believability of the SP in their role [11] and one explored both the SP experience and the impact on learners [13]. One paper stated that the older SPs were part of the research team and that the authors followed published reporting guidelines related to SP methodology [11]. All research reported human research ethics approval. All research articles had some component of qualitative research and for most, it was the primary focus. Research methods included observation in real time [13,21] or of recorded videos [11,21], written field notes [13], interviews [13,18], focus groups [20,22] and survey and other measurement instruments (e.g. evaluation forms, empathy scales) [14,16,21]. Four articles were educational guides involving SPs with a focus on learner outcomes [12,17,19,21] (Table 4).
| Year of publication | 2011–2016 [16,17,19,21] | 2017–2021 [11–15,18,20,22] | |||
| Country of origin | USA [11,12,14,15,17,19, 21] | Australia [13,16] | Canada [20] | Switzerland [18] | United Kingdom [22] |
| Focus of Journal | Educational focus [12,14,16,17,19,21] | Simulation focus [15,18,20,22] | Profession- specific focus [11] | Education and profession- specific focus [13] | |
| Learner group | Specific student groups [12,13,14,16,21,22] | Healthcare professional groups [15,17,19,21] | Not mentioned [11] | Not applicable [18,20] | |
| Article type | Research – Qualitative [13,15,18,20,22] | Research – Mixed methods [11,14,16] | Educational guide [12,17,19,21] |
SPs were described with language that included ‘standardized patient’ [11,12,14,19,22], ‘simulated patient’ [13,18] or ‘simulated participant’ [15,20]. Certain articles described the SP as both a ‘standardized patient’ and ‘actor’ [16], a ‘simulated patient’ and ‘actor’ [21] or a ‘simulated’ and ‘standardized patient’ [17].
Eight articles noted the specific age of the SPs, with an age range of 50–92 years old [11,13–15,18,20–22]. In one of these articles, the SPs’ age ranges were described as being between 50–70, so it was included [11]. Where a specific age was not noted, the SPs were described as being older adults [12], elderly [16], within ±5 years of the stated age of character (over 60) [17] or having an age that reflected the age of the person they were portraying (over 60) [19].
SP roles – that is, the information provided to the SP about the character to be portrayed – were all described as being some type of written document except for one study which indicated that role details were communicated to the SP through an oral briefing [14]. Where described, SP roles were called a blueprint [11], script [12,15,17] or scenario [19]. The articles that were educational guides provided the complete roles [12,17,19,21].
Information in the SP roles included identifying that the character, the person the SP was portraying, was a patient [11–17,19,22], the spouse of a patient [19] or a grandparent [21]. In five studies, the specific age of the character was reported, with the range of 60–92 years old [11,12,17,19,21]. In two studies, the characters were described as being elderly [14,16]. Other information included name [17,19], gender (either male or female) [11,12,15,17,19,21], current health status/disease state [11,12,14,15,17,19], social history [11,12,17,19], past medical history [12,17], mental state [19], medications [12,19], description of affect and/or behaviour [11,12], physical appearance [12,19], marital status [12,17,19], place of residence [12,16,17,19], degree of independence [12] and relationships with others [12,17,19,21]. Two articles specifically noted no restrictions on ‘race’ or ‘ethnicity’ [11,17]. Two articles described characters as having a specific religious background [17,19]. Two articles provided in-depth disease-specific characteristics (e.g. related to aphasia post-stroke or Parkinson’s disease [11] or hearing loss [21]).
Some roles also reported the inclusion of prompts or scripted lines/guidelines for the SP [12,15,16,19,21], detailed information about the medical condition, including symptoms and behavioural markers with specific examples [11,12,19,21], instructions for SPs about how to respond to different communication strategies used by learners [11,19] and a list of questions for SPs to ask and/or possible learner responses [13,19,21].
Within the scenarios – that is, the more encompassing documentation of a simulation session within which the SP role is located – information provided included the objectives of the simulation activity (e.g. stated aims and objectives, descriptions of desired outcomes or scenario overviews [12–17,19,21,22]). Settings were provided for all scenarios and related directly to the context and objectives, including medical/hospital areas (e.g. outpatient clinics or acute care) [11–15,21]; clients’/patients’ homes; nursing homes [16,19] or multiple settings across sectors [17,22].
Additional scenario information included: behaviours students were expected to demonstrate [11], an outline of the expected flow of the scenario [12,17,19], debriefing questions [12,17,19], patient charts, tests, forms, medication lists and/or assessment tools the learners were expected to use [14,17,19,21], different versions of the scenario (e.g. for students, faculty, SPs) [17,19,21], roles for other role players in the scenario [12,19] and evaluation forms [17,21]. Complete scenarios were provided in two articles, both descriptions of educational activities in MedEdPORTAL [17,21].
Three articles addressed development of the SP role and/or scenario [17,19,22]. Roles were based on actual cases/practices and either described an intervention [11], an educational process [19] or were an educational guide [17]. No articles directly noted SP co-development of the role or scenario, although some articles indicated that the SPs were encouraged to use personal details about themselves or their experiences in healthcare to enhance authenticity [13,21,22].
In six articles, recruitment processes included selecting SPs who were experienced, came from various backgrounds (e.g. clinical, education) and were members of SP programs [11,12,15–17,19]. One article mentioned that SPs were paid [11]. Other SPs were volunteers from communal living settings for older adults [13], or from the surrounding community [14], or users of healthcare services who started working as SPs, mostly by word-of-mouth referral [16]. One article noted that it was important that the SP be free of any signs or symptoms of the condition they were portraying [11]. Another article noted varying cognitive abilities of the SPs [13], and another referenced their frailty [15]. Two articles recommended the SP should look the age of the person they were portraying [17,19]. One article reported that the SP portraying the character with Parkinson’s disease should be male as this condition is more common in men [11].
SPs were trained by SP educators/trainers (SPTs) in two studies [15,17] and faculty researchers in one study [11]. The other studies did not state who trained the SPs.
In addition to the SP role, other training materials included: SP and learner assessment tools [11,17,19], general orientation materials related to the session content [15], SPs’ life experiences [13], videos of patients with conditions the SPs portrayed [11], videos of SPs rehearsing the role to self-assess readiness to perform the role [11] and videos of previous encounters between learners and SPs [6].
Training time, when reported, ranged from 30 minutes to 6 hours [11,14,15,17,19]. One article indicated that the training consisted of more than one session [11].
The goal of training the SPs was described as promoting a realistic presentation [11], making sure the SP felt comfortable portraying the role and had an opportunity to practice [12], helping the SP become comfortable with the simulation environment and providing them with the opportunity to ask questions [14] and working with them to refine their responses and affect [15]. One study provided a training checklist for SPTs to ensure that they thoroughly trained the older adult SPs, with consideration of both content and process, including standardization of role presentation [17].
The training formats were diverse. Some SPs received a script prior to the simulation session and/or a list of responses to anticipated questions from learners [12,16]. Training in two studies consisted of a verbal briefing about the case prior to the session [14,16]. One of these briefings also orientated SPs to the simulation environment and provided them with the opportunity to ask questions [14]. Some SPs were asked to prepare prior to the training by reading material related to the subject of the session [15]. Training sessions were described as offering the SPs the opportunity for practicing and feedback, although specific guidance for how to do this was not provided [11,15,17,19,22]. One study described faculty and SPs observing videos of their rehearsals to determine SP role-readiness [11]. Another study reported that SPs observed other SPs in actual sessions prior to portraying the role [22].
The total number of SPs recruited for each project was noted in six studies [11,13–15,17,21,22]. It was unclear if SPs were trained individually or in groups except for two reports: in one study, two SPs were trained for one role at the same time for standardization purposes [11]; in the other study, two SPs in their 80s, portraying a husband and wife, were trained with two other simulated family members [19]. Another study noted that students portrayed roles such as healthcare providers and a family member and were briefed individually just before the simulation. These students did not appear to have been trained with the SP [12].
Five articles indicated that the SPs participated in feedback with learners [12,13,17,19,22]. Of these articles, two mentioned that SPs provided verbal feedback [13,19], and one mentioned written feedback, also providing the assessment form used by the SPs [17]. One article indicated that the SP was present at the debriefing [21] while in another article, the SPs were reported as providing feedback and leading the debriefing [22]. In two other articles [12,13], although there was no feedback training mentioned, SPs were described as giving feedback. Details about feedback and debriefing training, such as how and when it was done, or how it unfolded during the simulation activity, were not provided in any articles, with the exception of the written assessment form [17].
Sessions were formative and described as being one-time events [14] or recurring sessions [12,13,15,16,19,21,22]. There was also a six-station formative Objective Structured Clinical Examination (OSCE) [17]. Two studies described hybrid simulations: one with SPs and task trainers [13] and another with an SP and a manikin [21]. One article featured a videotaped interview between an SP and a simulated doctor that was used for research [11]. Six articles indicated the number of SPs who participated in the activity [11,13,15,16,21,22]. Two articles did not explicitly state the number of SPs, but the number might be inferred based on context and the number of scenarios run at the same time [14,19]. Eight sessions were delivered to pairs or small groups of learners, some with faculty present [12–16,19,21,22]. The length of the SP interactions per encounter, when reported, ranged from a ‘few minutes’ to 75 minutes [11,13,14,17,19,21,22]. Two studies indicated that SPs portrayed their roles five [14] or six [17] times in a row; otherwise, this detail was not provided. One study described debriefing SPs separately after the simulation [13].
This review offers insights into what is known about older adults as SPs in healthcare education. Older adult SPs participate in a variety of simulation activities that reflect SP practices reported for the wider population. Articles that focused on learner outcomes [14,16] concluded that designing simulation activities related to the care of older people while working with older adult SPs enhances and supports healthcare professionals’ development of competencies. Articles that focused on SP-based outcomes [15,18,20,22] recommended the importance of involving and supporting older adult SPs in the educational design processes, while also ensuring their ongoing development and well-being. While some aspects of SP methodology were outlined in articles, overall, there was inconsistent reporting. Some articles did reference established simulation standards [13,15,18–20] or reporting guidelines [11], but many did not appear to build on what is already reported in the literature.
The limited reporting of details when working with older adult SPs could delay the intended application of such knowledge to the care of older people. This was emphasized in previous research about SP work [23] and simulation in general [24], along with suggested frameworks for reporting. From the research reporting guidelines developed by Cheng et al. [25], we recommend the minimum requirement for reporting on simulations involving older adults for the sub-element labelled Actors/confederates/standardized/simulated patients should include the age of SPs who played the role, the age of character/role, recruitment criteria and specific information related to training for role portrayal and for feedback. By improving the reporting details, we would also gain insight to the importance of aligning the age of the older adult SP with the role to be portrayed.
As expected, educational guides offered more detail about older adult SPs than the research articles. The latter were not necessarily focused on educational interventions. Templates for writing SP-based scenarios exist [26]. Some are evidence-based, and some are not. Based on a scoping review, Davies et al. [27] make recommendations for reporting in SP role templates. While their template is comprehensive, it is intentionally confined to information about SP role portrayal. Our review has identified that without broader contextual information (e.g. recruitment, training approaches for role portrayal and for feedback), of the educational activity, the template information alone is limited. We recommend guidelines offered for Educational Summary Reports at MedEdPORTAL when reporting on older adult SP educational activities [28].
The ethics of simulation practice has been highlighted [29,30], including the responsibility of considering the well-being of all those involved. The well-being of older adult SPs was addressed in varying degrees in some of the articles included in our review [14,15,18,20,22]. Of course, it is possible that the well-being of older adult SP was attended to, but simply not reported. Drawing on examples of included articles, there are risks when SPs portray themselves, using details from their own lives, or provide feedback without having been provided with any parameters or support. SPs may include details that could be potentially triggering for them or learners, or may have nothing to do with the learning objectives, and therefore prove to be a distraction. Current standards for SP methodology [6] support a ‘safe psychological and physical learning environment’ such as screening criteria. For older adult SPs, screening considerations would include their current circumstances and their cognitive and physical suitability to undertake roles [7]. These considerations are especially important if roles involve potentially distressing situations, or if there are lengthy, detailed scripts with complex behavioural affects. There is also the potential for fatigue through constant repetition of role portrayal or through the combination of role portrayal with additional tasks such as feedback and written assessments. Suggestions to have dedicated individuals (e.g. SP educators/trainers) to support older SPs’ valuable contribution were echoed in four of the articles [17,18,20,22].
From the details provided, there appeared to be little diversity in the characters and situations contained in the articles, including ethnicity, culture and other social determinants of health; all derived from first authors in the Global North. Only two articles mentioned ethnicity: one noted that although SPs of any background could be recruited, the SPs recruited were ‘white’ [11]; the other mentioned that in the future, families from various ‘ethnic groups’ could be recruited [19]. The characters portrayed in the simulations appeared to be middle class. This lack of detail related to diversity in the role/scenario and recruitment instructions for the SPs is reflective of reports in broader simulation practices [31–33]. In response, simulation educators are increasingly focused on ideas and recommendations for supporting the creation of scenarios that feature inclusion of SPs across the simulation design process and the recruitment of more diverse SPs to portray those represented [34,35].
Words matter and in working with older adult SPs, it starts with the way adults over the age of 60 years old are described. We have adopted the age of 60 and the term older adult from globally acknowledged organizations [1,2]. The American Medical Association [36] notes that the word ‘older’ is a respectful and neutral way of referring to adults in this age group rather than using terms such as ‘elderly’, ‘senior’ or ‘the aged’ which can ‘… connote discrimination and certain negative stereotypes that may undercut research-based recommendations for better serving our needs as we age’ ([36] p1386). We also recommend critical reflection of other terms used to describe the living spaces of older adults while also recognizing that terms will vary across countries. The American Gerontological Society offers recommendations for various terms [36]. It was also surprising to see that the term ‘standardized patient’ was the most prevalent one used to describe the acronym SP, despite international advocacy for ‘simulated participant’ [6,37], a more inclusive phrase that reflects the person-centred presentation of older peoples’ journeys in healthcare, one that can include patients, carers, family members and others. Some articles also referred to ‘using’ SPs, or ‘utilizing’ SPs, which signals that SPs may be seen as tools rather than as agentic members of an educational team. There has long been critique of this objectification of SPs with recommendations for ‘working with’ or ‘engaging with’ SPs as a more productive way to position their valuable contributions [38,39].
Our search strategy focused on three conventional databases, articles written in the English language, plus a limited search for other articles in the reference lists of included articles, MedEdPORTAL and Google Scholar. However, we needed to balance the number of potential sources with the resources we had for screening them. There was a missed opportunity to include many articles because it was unclear if older SPs were involved. During the review, we also noted that one of the terms used in our search strategy, ‘simulation-based education’ (SBE) is also called ‘clinical simulation exercise’ (CSE) in some nursing and interprofessional papers. We may have missed some relevant articles as we did not use this term. Establishing consensus on terms used to describe this type of education across disciplines and professions would be helpful. It is also possible that the makeup of our research team impacted the findings; however, we attempted to mitigate biases by following Arksey and O’Malley’s framework.
SBE related to the care of older adults is increasingly important as our population ages. Older adult SPs may contribute to healthcare providers training in authentic, engaging, safe and effective ways. This scoping review provides a foundation on which to further develop older adult SP practices by highlighting their well-being and safety (both physical and psychological), promoting ways to increase diversity and inclusion, and emphasizing that the words we use matter. Improved reporting details of articles involving older adult SPs will facilitate the identification of effective practices. Research to support both learner-centred and older SP-focused approaches is important to promote meaningful simulation-based learning in the care of older people.
The authors would like to thank Tonya Mahar, Manager, Library Services at Baycrest and Sarah Bateup, Faculty Librarian, Health Sciences and Medicine, Bond University for their support with the literature searches. We also want to thank the older adult SPs who inspire us everyday.
All authors contributed equally to this study.
None declared.
Database available from corresponding author upon request.
Not relevant.
The authors declare no conflict of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
 Exploring the content validity of Clinical Cultural Competence Questionnaire in diverse cultures
Exploring the content validity of Clinical Cultural Competence Questionnaire in diverse cultures
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets