
Caregivers of persons with dementia (PWD) frequently face physical assault and emotional abuse when providing care. Providing experiential opportunities for caregivers to develop skills that maximize safe, compassionate care is a priority. Human simulation has demonstrated greater effectiveness than didactic activities in developing clinical skills. However, this requires consideration of physical safety for both learners and simulated participants (SPs), limiting the full expression of behaviours. To address this limitation, we conducted a proof-of-concept study engaging SPs on a synchronous, facilitated VR platform responding realistically, but safely, to learners’ communication approaches. Learners negotiated online with potential threats of violence from the SPs.
This study used a pre/post mixed-method research design. Both qualitative and quantitative approaches were used to explore the impact of this training on participants’ knowledge, confidence and comfort when providing care to PWD.
Overall, participant ratings of knowledge, confidence and comfort increased post-training, as compared to pre-training (p = 0.28, p = 0.26 and p = 0.70, respectively). Although these increases were not statistically significant, the results were consistent with qualitative data related to these outcomes. However, after adjusting for participants’ prior training in working with PWD, significant increases were associated with the subgroup of novice learners but not for the subgroup who had previous experience (interaction p = 0.004, p = 0.03 and p = 0.02, respectively).
Our findings provide insights into the implications of VR-based training for managing responsive behaviours of PWD. VR training has the ability to increase caregiver knowledge, confidence and comfort working with PWD who are exhibiting responsive behaviours, as shown by participants.
What this study adds
According to a 2015 report conducted by Health Quality Ontario (HQO), approximately 70% of seniors living in long-term care homes are diagnosed with dementia [1,2]. Caregivers of persons with dementia (PWD) frequently face physical assault and emotional abuse [3,4]. Many formal caregivers accept abuse from PWD as ‘part of the job’ [5] and some note that the abuse can affect their ability to provide client-centred care [4,6]. Specifically, caregivers report physical injury, psychological distress, reduced job satisfaction, burnout and increased feelings of anger, sadness, guilt and helplessness [4]. Caregivers across various contexts, including hospital, long-term and home care, are at risk of harm due to situations that escalate both verbally and physically. In an Australian study of calls to a hospital Aggression Response Team, 72% of patients involved had underlying dementia and 88% of those cases were resolved with pharmacological sedation [7]. Pharmacological sedation and/or physical restraint interventions carry significant risk to patients [7,8]. Consequently, many organizations have adopted least-restraint and minimum sedation policies and have emphasized verbal de-escalation techniques to manage responsive behaviours (e.g. physical aggression), which are thought to be expressions of unmet needs [9]. Caregivers require practice of strategies and competencies in verbal conflict de-escalation and situational awareness to maintain physical and psychological safety for themselves and their patients [3,6,7].
Current training for caregivers of PWD is primarily achieved through didactic activities such as online courses, which limit learners from applying their skills experientially (e.g. via simulations), and discussing or debriefing about their training. While simulation has been demonstrated to be more effective than didactic activities in developing clinical skills across many healthcare contexts [10], our experience suggests that in-person simulation has significant limitations for the training of de-escalation skills. First, the full expression of responsive behaviours must be limited to ensure that both learners and simulated participants (SPs) are not physically harmed. For example, within in-person settings, we train SPs to refrain from engaging with environmental artefacts such as canes and ID badges that would pose a potential threat to the safety of both the PWD and care provider. The anecdotal and post-simulation survey feedback we have collected to date from in-person simulations suggests that this limits the effectiveness of training, as learners are not able to fully experience the management of complex behaviours that risk progressing to physical threat. Second, administration of in-person simulation is resource-intensive with access typically limited to large urban centres [11,12]. Finally, learners in live simulation sessions do not have the opportunity to fully experience the perspective of the patient, limiting the potential for development of empathy. While previous work in virtual reality (VR) dementia simulations has demonstrated that taking different perspectives helps build empathy towards both the caregiver and the PWD [13], VR solutions to date have not leveraged a human SP in a synchronous, facilitated simulation, which limits the ability to explore complex behaviours.
To address the limitations of conventional simulation, we conducted a proof of concept study which engaged a VR platform and simulation curriculum focused on training healthcare workers and students in the de-escalation of responsive behaviours. We evaluated the usability and feasibility of a novel VR platform and simulation curriculum for the de-escalation of responsive behaviours. Specifically, we designed a VR de-escalation platform that allows an SP to use their environment to introduce a realistic (but safe) threat of violence if the situation called for it. For example, an SP can swing a virtual cane in response to a learner who is exhibiting ineffective communication skills. Further, we designed the platform to show multiple perspectives (caregiver, patient and bystander) for observers of the simulation. In particular, the patient’s perspective was included to build empathy and contextual understanding. An additional goal was to enable remote simulation in a VR environment to increase learner access and opportunity.
The VR platform was developed by the Ottawa Hospital Research Institute, and was a headset-based, virtual clinical environment populated by one SP (portraying the PWD) and one participant (portraying the caregiver), both represented as 3D avatars. The environment was designed using the Unity3D (Unity Technology, San Francisco, California, USA) development environment. The system was created to be compatible with SteamVR-based VR systems (Valve Corporation, Bellevue, Washington, USA). For our study, we leveraged the Quest headset (Meta, Menlo Park, California, USA) tethered to a PC with a dedicated graphics processing unit (Nvidia, Santa Clara, California, USA) for both the SP and participant. Remote interactions between users were coordinated using the Photon PUN (Photon Engine, Hamburg, Germany) plugin and cloud service. For non-participant observers (those learners who did not wear the VR headset), this platform provided 2D views of the patient’s perspective, the caregiver’s perspective and a global ‘bystander’ perspective as shown in Figure 1.

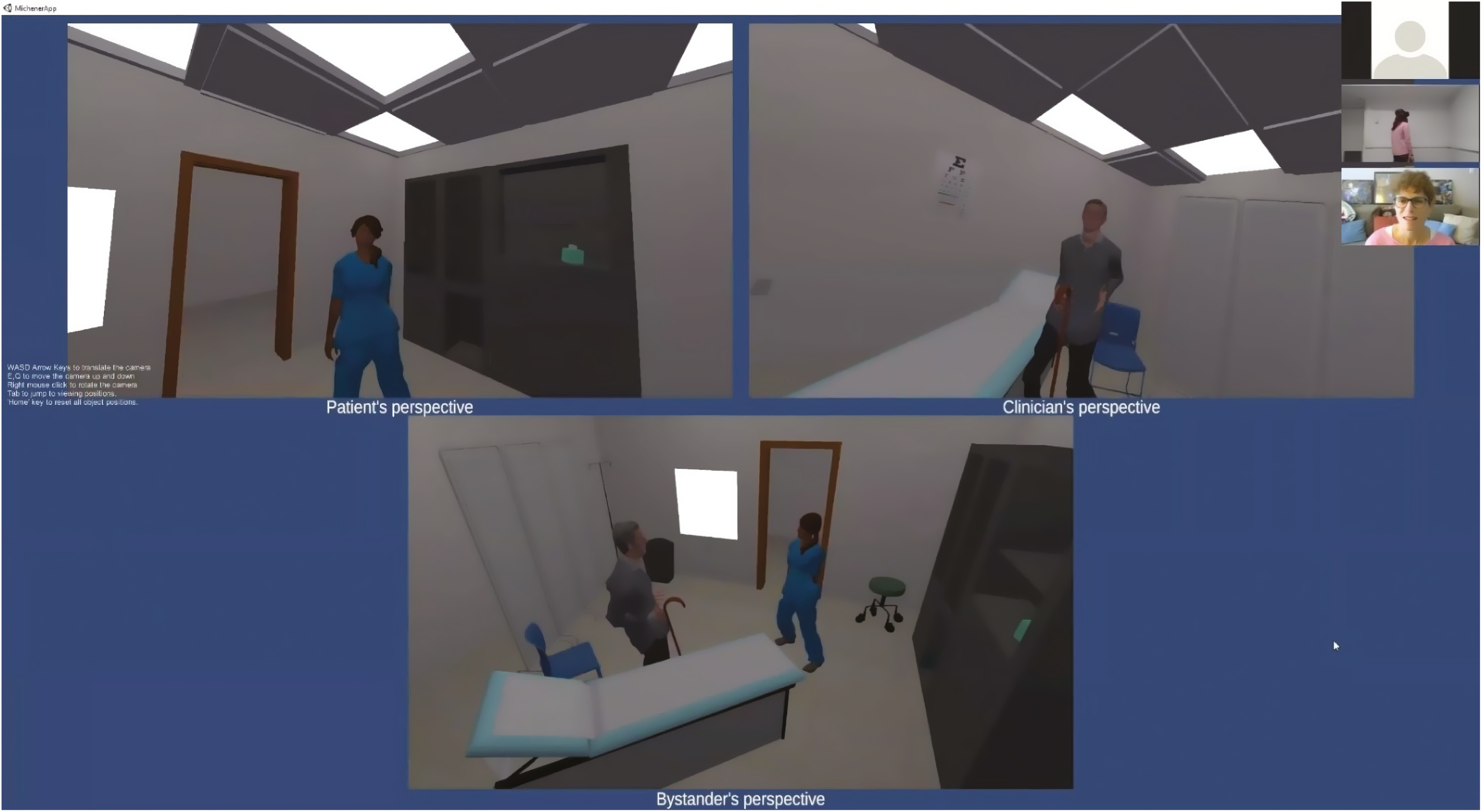
Multiple-perspectives observer view of verbal de-escalation in VR.
This study used a pre/post mixed-method research design [1]. Both qualitative and quantitative approaches were used to explore the impact of this training on participants’ knowledge, comfort and confidence when providing care to PWD, as well as feedback on usability and feasibility.
Fifteen clinical staff and students at Baycrest (a geriatric health system in Toronto, Canada) consented to participate in the study. Four individuals were unable to attend the scheduled training sessions and therefore, only 11 individuals completed the training and post-training surveys. Participants were required to complete Baycrest’s existing annual didactic online training module about responsive behaviours prior to the VR simulation training session, so they could compare this conventional training with the simulation-based VR-based training during qualitative data collection.
A third (33.3% of 15) of the study participants were nurses or other allied health professionals. Another third (33.3%) were feeding assistants and the remaining third (33.3%) were healthcare students, residents or interns. Most participants (60.0%) had a college or undergraduate university education while the remaining (40.0%) had a graduate school education.
Study participants had a median of 4 years’ work experience since graduation (interquartile range 2–12 years) and a median of 2 years working with PWD (interquartile range 1–6 years). Most of the participants (80%) needed to use de-escalation strategies in their current occupation and the remaining 20% indicated they might use these strategies. Approximately 67% indicated they had received training to work with PWD; however, 33% had not received that type of training.
The curriculum for the simulation scenarios was based on live behaviour de-escalation training usually provided for new staff at University Health Network (UHN) in Toronto, Ontario, Canada. The scenario was slightly modified to focus on an older person with dementia. The scenario had the following learning objectives:
Two simulation sessions were held: the first on 14 December 2020 (N = 6), and the second on 21 January 2021 (N = 5). During the simulation, participants either wore the VR headset (N = 4) and interacted synchronously and virtually with the SP (both as avatars in a VR space) or observed the VR interaction via Zoom (N = 7) (Zoom Video Communications, Inc., San Jose, California, USA). Figure 2 outlines the methods by which participants were divided between in-headset VR roles and observation roles via Zoom. SPs were experienced with live simulations of behaviour de-escalation. Prior to the simulation, the VR headset participants were provided approximately 20 minutes of training to orient them to the headset, hand controls, the virtual environment and the process to call a ‘time out’ if needed. The observer participants were oriented to three 2D perspectives (Figure 1) available to them throughout the session. Lastly, all participants were briefed about the scenario which revolved around a PWD (SP) attending an appointment in a clinic. The VR headset participant was directed to use different strategies and de-escalation techniques to manage any responsive behaviours. The simulation involved a PWD who was brought to the clinic for a follow-up appointment by his caregiver. The caregiver had left the patient alone momentarily to get him something to eat. The participant entered the room to find the patient confused and alone. During the scenario, the SP demonstrated responsive behaviours and modified their behaviour based on the actions of the participant. Immediately following the session, a trained facilitator and the SP debriefed with all the participants via Zoom. The debrief was conducted by a trained facilitator with experience in similar in-person simulations. The debrief script is outlined in Box 1. The SPs were also invited to provide feedback to the VR headset participant. After one simulation was completed, a second simulation with the same scenario but increased stress and responsive behaviours was run with another VR headset participant. A debrief was also held after the second simulation.
Box 1: Debrief Script
The debrief will be conducted in Zoom. Following the simulation, direct the SP and the VR participant to take off their VR headset and switch to the computer’s integrated mic/speakers or a dedicated headphone/mic. The facilitator and participant should start with webcams on, and the SP should turn on her camera when commencing feedback.
Facilitator’s script:
1. How was that for you? How did that feel? What worked well? What were some of the obstacles? Were there any surprises? I appreciated/noticed when you were able to …
2. ‘I’d like to introduce you to our SP ____________ and ask them to give you some feedback about their experience in this encounter with you’. SP FEEDBACK
3. (to the Observers) What did you appreciate seeing your colleague ___________do or say in this encounter?
4. Back to the learner. Is there anything you said or did that might change for in the future?
5. Have you ever encountered something like this in your own practice? What kinds of skills or techniques can you take from today’s session back into your practice?
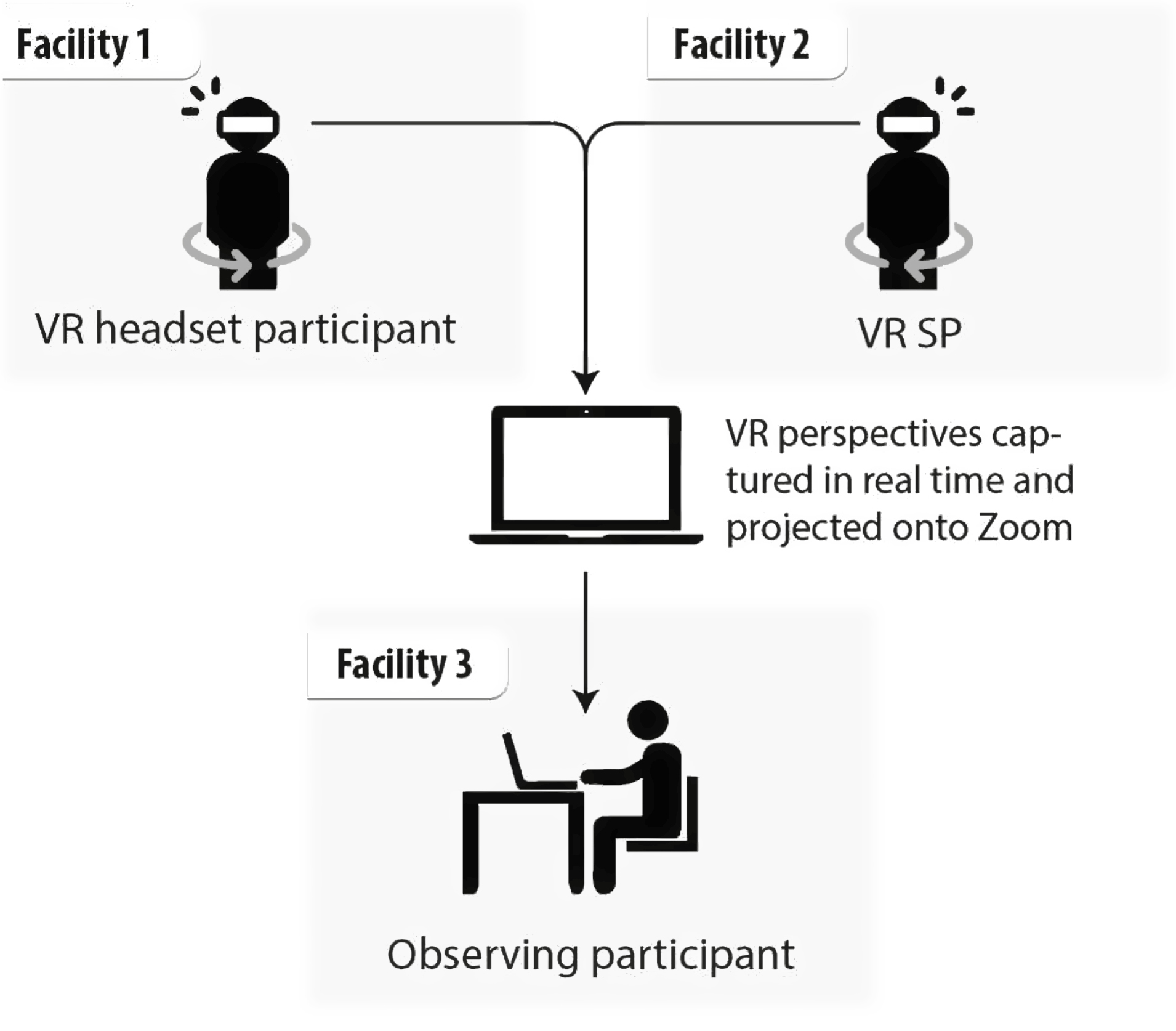
Division of in-headset VR and Zoom observation roles.
Participants rated their knowledge, confidence in care and comfort when caring for PWD both before and after their VR de-escalation training via a survey administered through REDCap (Vanderbilt University, Nashville, Tennessee, USA). They also had the opportunity to provide qualitative feedback on open-ended survey questions and through interviews/focus groups. Demographic information was collected pre-training through a questionnaire.
Five semi-structured interviews were conducted to provide more detailed feedback about participants’ experience; two with VR headset participants and three who had observed the simulation via Zoom. One focus group was held with four participants (two VR headset participants and two Zoom observers). These sessions were audio-taped and transcribed by research staff using InqScribe (InQuirium, Chicago, Illinois, USA).
It was hypothesized a priori that the VR training would increase knowledge about strategies for managing responsive behaviours, comfort working with PWD and confidence in the ability to apply strategies to manage responsive behaviours. Changes in the participants’ self-ratings related to knowledge, comfort and confidence (ranging from 0 to 100) were the primary outcomes and were measured pre and post the VR training session. The overall ‘level of satisfaction with the training’ rating (ranging from 0 to 100) was a secondary outcome and was measured post the VR training session.
Descriptive summaries include means, standard deviations (SDs), proportions, interquartile ranges and Pearson correlation coefficients. The primary outcomes of knowledge, confidence and comfort post-training were analysed using linear mixed-effect models. A random intercept with a variance components structure was included in the model to adjust for correlations between the pre- and post-measures within participant. All 15 participants were included in the analysis with 11 of the 15 completing both pre- and post-measures and 4 completing only pre-measures. All models were adjusted for time with the pre-measures as the reference value and additional models also adjusted for prior training to work with PWD (yes or no) and included an interaction term between time and prior training. Model estimates of mean ratings are standardized by SD of the pre-measures and include 95% confidence intervals. No adjustments were made for multiple testing. The data analysis for this paper was generated using SAS/STAT software version 15.2 and the SAS System for Windows version 9.4. Copyright © 2016 SAS Institute Inc.
Qualitative data were initially coded by one researcher (NM) and verified by another (JH). Thematic analysis was used to identify, examine and interpret themes inductively. Coding categories were organized using an iterative process of analyses. Thematic analysis is a method for identifying, analysing and reporting patterns (themes) within data. It minimally organizes and describes a data set in rich detail [14].
Overall, participant ratings increased in knowledge, confidence and comfort post-training, as compared to pre-training (p = 0.28, p = 0.26 and p = 0.70, respectively). Although these increases were not statistically significant, the results were consistent with qualitative data related to these outcomes. However, after adjusting for participants’ prior training in working with PWD, significant increases were associated with the subgroup of novice learners but not for the subgroup who had previous experience (interaction p = 0.004, 0.03 and 0.02, respectively, Figure 3).
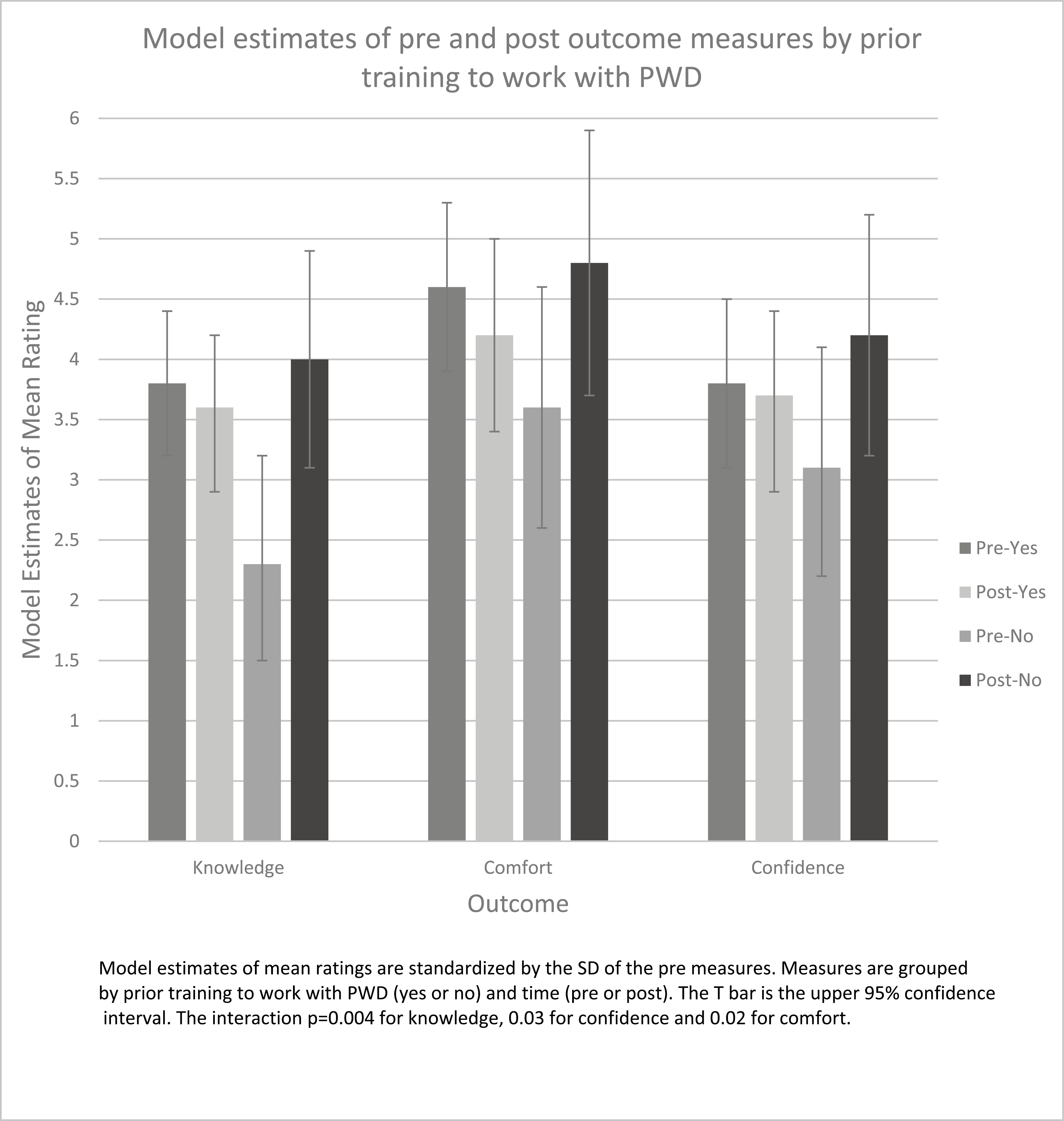
Model estimates of pre- and post-outcome measures by prior training to work with PWD.
Participants commented that the training supported integration and application of their clinical knowledge in a simulated practice setting, as exemplified in the following quote: ‘It’s practical learning, it’s audio-visual learning that you grasp, so it just sticks in your mind in a lot of ways because a lot of your different aspects of your memory are associated with’ (Int. 103, line 63–66). ‘I could feel the emotion and what was going on… if he’s going to hit hurt her, is he going to be de-escalated or not. So that was very, that felt quite real’ (Int. 103, line 28). ‘And so, the learning is just so immersive when it’s left to you to make those kinds of decisions, right? Like they could have observed the nursing staff a hundred times and still like, you know, when you are forced to be the one to do it, I think it just brings learning to the next level’ (FG, line 78–80).
Forty-five per cent of participants reported increased confidence after the VR training with 100% of participants in the ‘novice learners’ subgroup reporting increased confidence. Participants noted that the VR training increased their confidence in their daily practice when caring for PWD. ‘It provided interesting discussion which gave me great ideas about de-escalation tactics to employ in my daily practice’ (Int. 107, line 45). Comments reflected similar appreciation for the value of VR simulation training for increasing confidence in practice settings. ‘I think I know stuff, but I need more practice. But I generally feel doing something like that would give people more confidence’ (Int. 108, line 68).
Interview/focus group comments supported the questionnaire responses and also reflected participants’ comfort regarding the nature of the learning environment. For example, ‘The simulation felt real, support was offered before, during and after the simulation. It is a great experience for inexperienced individuals’ (Int. 107, line 120). ‘So with VR, I think that’s going to create a lot of comfort zone for the trainees to be in that, in that scenario, and learn first-hand from those experiences...’ (Int. 103, line. 113).
Qualitative analysis showed that participants felt supported in the learning environment during the VR training.
Participants reported high engagement (average = 90.2/100), high satisfaction with the VR training (average = 87.3/100) and high authenticity (average = 76.7/100). The average authenticity rating was positively associated with participants’ satisfaction with the VR training (correlation coefficient = 0.76, p = 0.006, n = 11). Participants remarked on the emotional nature of the learning in the VR simulation, both in the descriptive post-training responses as well as the interviews/focus groups. They commented on feelings that the VR simulation successfully evoked, using words like ‘frustrating’ and ‘anxiety’, suggesting that the real feeling created by the VR was an important factor in their learning experience: ‘The simulations triggered memories of my own experiences, as well as what I learned during school and completing the e-module. I was empathic to the clinician and resident in the scenario because it can frustrating for both parties if they feel like they are not being heard or understood’ (FG, line 101–103). ‘I think it was pretty obvious that at one point I jumped out of my skin, [Laughter] that was very realistic’ (FG, line 104).
All participants recommended the VR training for other healthcare providers, both in the interview responses as well as the post-training questionnaires. A majority (54.5% of 11) would prefer the VR training as the training method for application in their work and the remaining considered both the VR training and Baycrest’s standard online training on responsive behaviours to be useful.
The majority of observer participants reported they frequently switched between observing all of the perspectives. Only a few watched the bystander’s or clinician’s perspective only. ‘I really appreciated having three different perspectives as an observer. So, being able to see everything through the clinician’s eyes, through the patient’s eyes, and then just move over bird’s eye view, I really liked that’ (FG, line 31–33).
‘I kept going back-and-forth and then occasionally I would look down to the bird’s eye, to see how close they were in relation to each other or like what elements of the room were potentially involved, or could be triggers or hazards, what it was, it was back-and-forth between the-the two participants’ (FG, line 39–41).
Our findings provide important insights into the implications of VR-based training for managing responsive behaviours of PWD. The findings demonstrate that our VR training has the ability to increase caregiver knowledge, confidence and comfort working with PWD who are exhibiting responsive behaviours, as shown by participants’ self-reports of changes. These findings are particularly relevant for long-term care where there is a high prevalence of responsive behaviours, especially in persons living with cognitive impairment [9]. Effective staff education and training that have been shown to impact these outcomes are necessary to optimize care [15].
Another interpretation of the results revealed that the level of a learner’s experience is important. The greatest impact was found in a subgroup of participants who had no experience with PWD. This suggests that our VR tool, in its current iteration, may be especially effective for early training of novice/trainee clinicians. This is consistent with findings from another recent virtual project related to responsive behaviours where participants with little knowledge (students) demonstrated significant increases in confidence identifying possible triggers and mitigating strategies, while practicing clinicians did not report similar changes [16]. Future development could focus on scaffolding learning by building curriculum that involves multiple simulations, moving from simple to more challenging presentations based on the one used in this pilot.
The implications of our secondary outcome results will also guide our next steps. Participants reported high satisfaction, engagement and authenticity. These results are important to note for the purposes of usability and feasibility of this type of training. The high ratings of authenticity, comments about the immersive and visceral nature of VR, and the ability to switch between the perspectives of the roles in the simulation all support our goal of empathy-building in clinicians. Our VR training revealed potential for empathy-building, both in those who wore the VR headset and those who observed. There is potential for improving empathy, even remotely using such a system. Satisfaction was also positively correlated with ratings of authenticity, which suggests that the environmental fidelity available through VR is an important factor for learner satisfaction.
Additionally, as all participants reported that they would recommend this VR training to other healthcare providers, these results are promising for future scaling and adoption of such training. It was also encouraging that no participants reported cybersickness due to VR (e.g. see [17]), which speaks to the quality of the VR platform we developed. Particularly notable is that this pilot happened despite the pandemic and consisted of a facilitator and SP joining the simulation off-site, in addition to allowing for remote participants. This suggests our VR training could be feasible and cost-effective for any healthcare organizations with access to the internet.
Some qualitative comments alluded to the current limitations of VR as a simulation modality. For example, one participant noted that her first instinct upon encountering the PWD in VR was to offer them a chair and sit down across from them at eye level. Due to the limitations of our VR platform, i.e. that artefacts of the physical environment cannot be dynamically integrated into the VR environment, transitioning from standing to sitting was not possible to do safely. Consequently, the participant felt that she was not able to authentically leverage her full skillset for managing responsive behaviours and was somewhat frustrated. While we designed the scenario and trained the SP to direct the encounter away from any transitions between sitting and standing, this is an example of how simulation-based educators must account for the limitations of VR (or any simulation modality) when determining fit-for-purpose: at best, the limitations are accounted for/designed around without affecting the learning outcomes; at worst, educators risk negative transfer by artificially limiting the full range of behavioural and clinical tools available to the learner [18,19].
It should be noted that these interpretations are preliminary. As a result of restricted research due to the pandemic, the number of participants was small which resulted in limited statistical power and generalizability. Further large-scale research with more robust experimental designs (e.g. with a control group engaging in conventional in-person simulation) and deep qualitative inquiry are required to advance the nascent field of VR-based simulation. Another limitation was the amount of time given to participants before entering the virtual space. Orientation to wearing the headset, using the hand controls and becoming familiar with the virtual space was limited to 20 minutes. Allowing for more time may have impacted the overall experience.
Our study focused on providing a similar (though augmented and remote-enabled) learning environment to in-person, facilitated, SP-based simulation. Though this was a deliberate design consideration, the synchronous and facilitated nature of our solution can be perceived as a limitation as well. Human SPs and facilitators are required, which incurs significant cost and limits access for education programs that are attempting to scale training opportunities. Recent advances in natural language processing and generative artificial intelligence [20] may offer future avenues for the training of complex behavioural competencies in fully asynchronous VR-based platforms that could provide effective feedback without the need for a trained facilitator or human SP. However, our team remains confident that facilitated, SP-based simulation will continue to be a mainstay education methodology for the foreseeable future due to the emergent and complex nature of healthcare training requirements.
Our research suggests that VR simulation with live SPs interacting synchronously provides a unique experiential opportunity for caregivers of PWD to develop skills that maximize safe, compassionate and responsive care. VR has the potential to reproduce highly contextualized practice environments that allow for simulation participants to explore dimensions of practice that may be difficult or impossible to achieve with conventional simulation. However, there are limitations to current VR technology that can also limit the environmental and conceptual fidelity of the simulation, and careful attention must be given to the alignment of learning objectives with the capabilities of the technology. Robust participant orientation to VR technology is essential. Overall, VR is an incredibly promising simulation modality, especially for novice learners.
The authors would like to thank our facilitators, Beverley Kramer and Kerry Knickle, and our simulated participant, Kerri Weir, all three of whom also provided feedback about the simulation. We would also like to thank Aideen Carroll from University Health Network for her contributions to the original in-person de-escalation scenario development. Special thanks to Justin Sutherland and the team at the Ottawa Hospital Research Institute for developing the VR platform and their collaboration on this project.
All authors contributed equally to this study.
This study was funded through a SPARK grant provided by the Centre for Aging and Brain Health Innovation (CABHI), award #SPARK-4-00278. This study was supported by the Centre for Learning, Innovation, and Simulation at The Michener Institute at University Health Network and the Centre for Research and Education at Baycrest.
De-identified data available from authors upon reasonable request.
The study was approved by Baycrest’s Research Ethics Board (REB# 20-23). All participants provided written informed consent.
The authors all declare no conflicts of interest.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
 VR-based simulation training for de-escalation of responsive behaviours in persons with dementia: efficacy and feasibility
VR-based simulation training for de-escalation of responsive behaviours in persons with dementia: efficacy and feasibility
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp

 Tweets
Tweets