
Responsive behaviours (e.g. physical aggression and agitation), often thought to be expressions of an unmet need, are common in persons with dementia (PWD) [1]. These behaviours may affect up to 90% of PWD over the course of their illness; are independently associated with poor outcomes, patient and caregiver distress, hospitalization and increased healthcare costs [2]; and pose safety risks. They are extremely challenging to manage, often because potential triggers are not recognized. There is a need for educational tools that help healthcare workers, students and caregivers identify and modify environmental factors that can contribute to responsive behaviours.
Education about dementia and behaviours typically occurs through lectures and printed materials. However, virtual dementia simulations, especially those designed to increase empathy, can be effective [3]. When compared with traditional education, virtual reality may improve post-intervention knowledge and skills outcomes of health professionals [4]. More research into immersive virtual learning in dementia is recommended [5].
Previously, we delivered an immersive ‘trigger room’ educational activity in person, where participants would observe a room and identify possible triggers for responsive behaviours. To increase accessibility and reach, we developed an online version using 360° illustrations and audio. The 360° format allows people to explore the virtual space as if they were actually standing in the room and better appreciate the environmental triggers highlighted in the tour. The rooms were drawn in Adobe Illustrator (Adobe, San Jose, California, USA), based on 360° photographs, and were made using simple line drawings in a monochromatic tone in order to minimize cognitive load. 3D Vista (3DVista, Grenada, Spain) was used to compose the 360° environment and interactions (i.e. identifying triggers, answering questions and moving between the rooms).
In the activity, participants virtually navigate through three simulated rooms of an older adult’s home (sitting room, bedroom and bathroom). The tour is self-guided and non-linear so participants can work at their own pace moving freely from room to room. The activity takes about 15 minutes to complete. There are twelve triggers dispersed amongst three rooms. Participants identify if each item could be a trigger (Figure 1). For those that are possible triggers, participants then select an intervention strategy from a list (Figure 2). The triggers and strategies were selected, reviewed and vetted by experts in the areas of Neuropsychology, Speech-Language Pathology and Geriatric Psychiatry who have experience working with PWD.

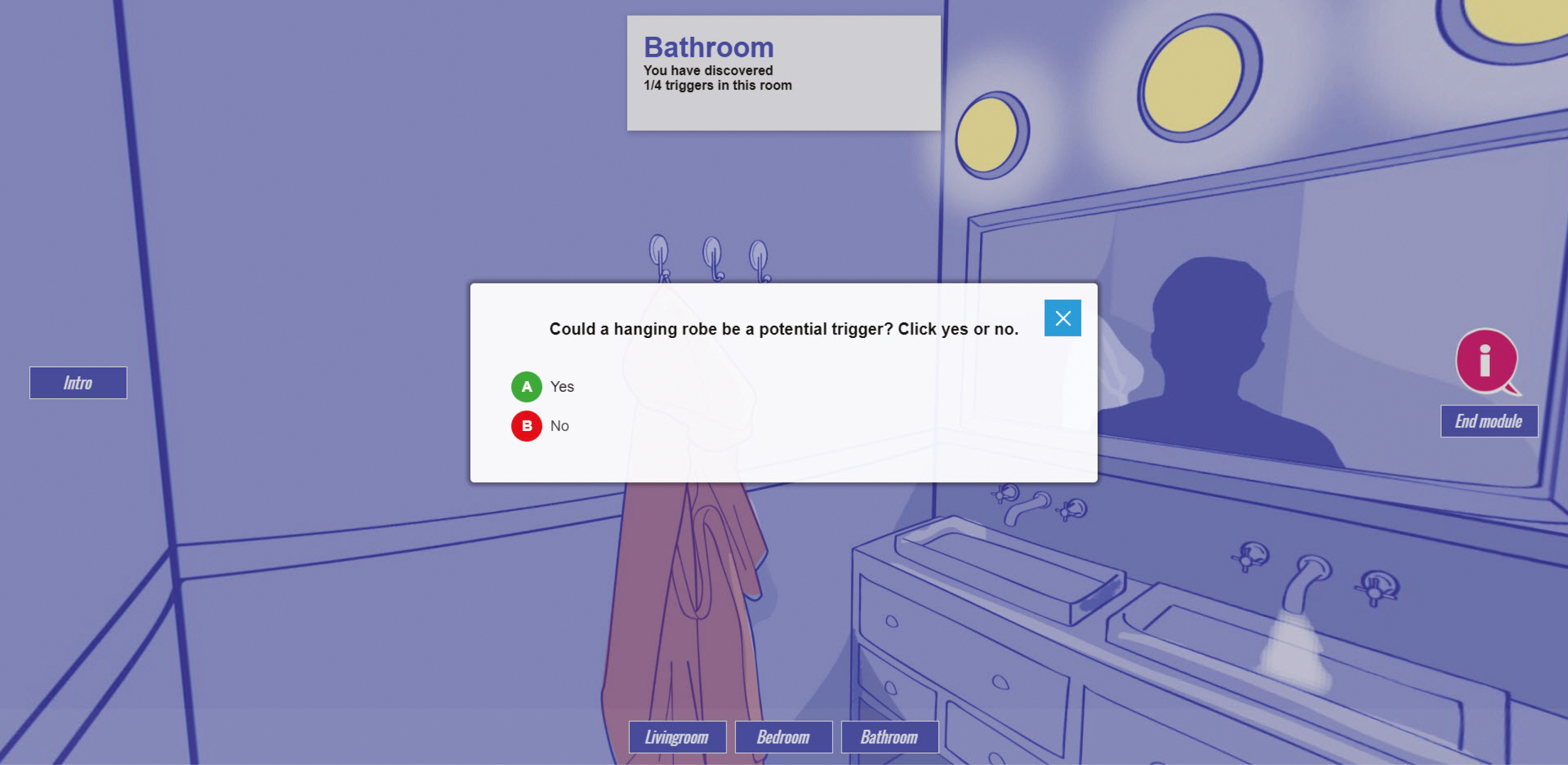
Example of choice of possible trigger
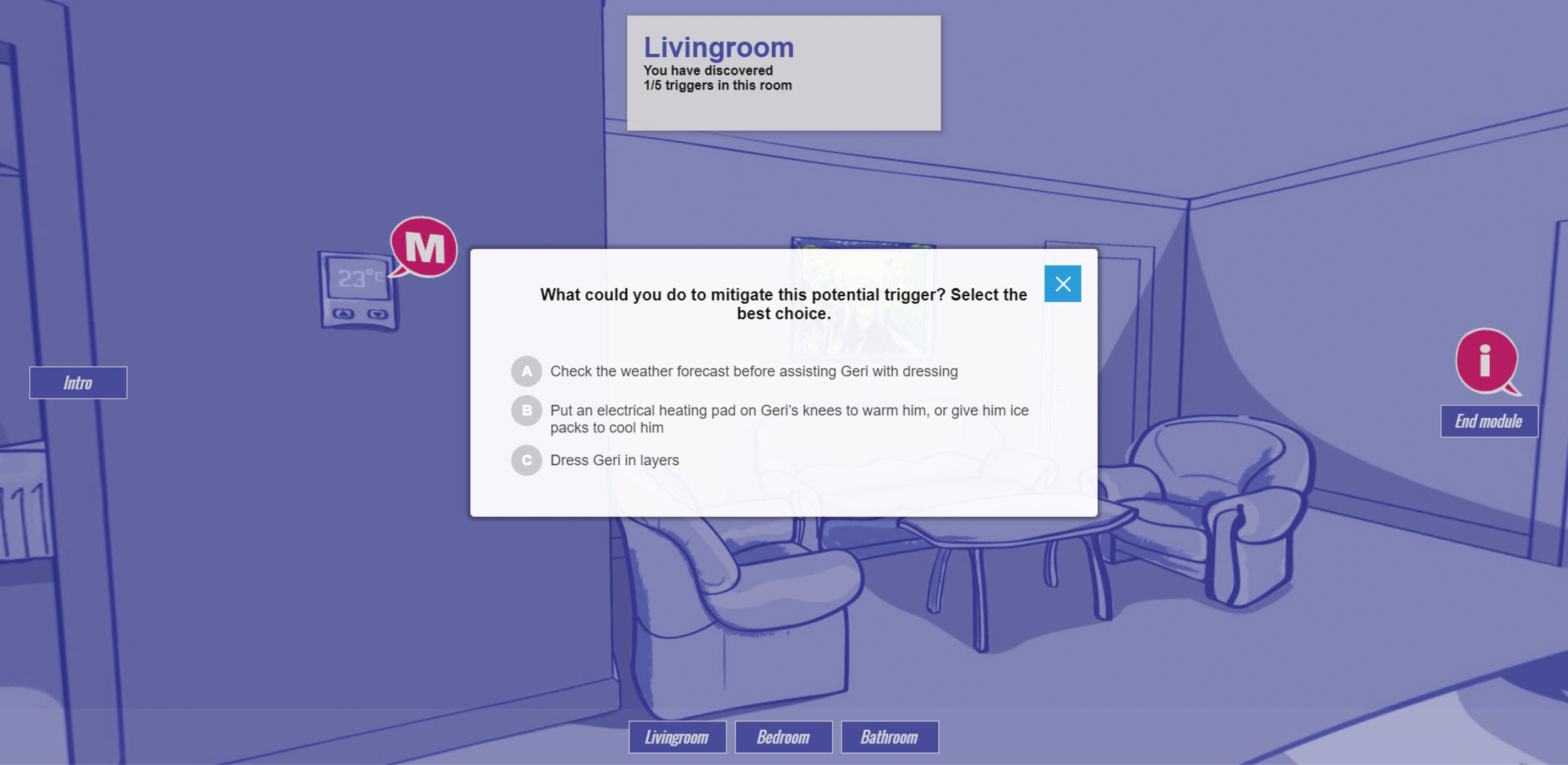
Example of choice of strategy
The virtual trigger room simulation is best accessed through a computer or tablet. It is hosted on Amazon Web Services (Amazon, Seattle, Washington, USA), for easy access to anyone with an internet connection.
Surveys were used before and after the simulation and captured quantitative and qualitative data. A total of 21 community healthcare providers and 62 students in Ontario college or university healthcare programs completed the activity and the evaluation. Descriptive statistics were used to summarize participant characteristics and survey responses.
The surveys included demographic information and asked participants to rate their knowledge about responsive behaviours and confidence in their ability to recognize environmental triggers and mitigation strategies at both pre- and post-simulation. To assess user experience and feasibility, there were also questions about participants’ satisfaction with the educational activity and suggestions for improvement.
Pre- and post-survey data were analyzed through the Wilcoxon signed-rank test, and the effect size (ES) was calculated as  , which is the corresponding effect size for this test involving small samples. The z-value is obtained from the p-value of the Wilcoxon signed-rank test statistic and n represents the number of respondents. Statistical analysis was performed using the SAS System for Windows version 9.4. (Copyright© 2002–2012 SAS Institute Inc.). Open-text responses from the survey were analyzed to determine prevalent themes using NVivo 11 (QSR International Pty Ltd, Doncaster, Australia).
, which is the corresponding effect size for this test involving small samples. The z-value is obtained from the p-value of the Wilcoxon signed-rank test statistic and n represents the number of respondents. Statistical analysis was performed using the SAS System for Windows version 9.4. (Copyright© 2002–2012 SAS Institute Inc.). Open-text responses from the survey were analyzed to determine prevalent themes using NVivo 11 (QSR International Pty Ltd, Doncaster, Australia).
Students: there was a significant increase from pre to post measures in a) self-reported levels of knowledge about responsive behaviours, b) confidence in their ability to recognize environmental triggers and c) recognition of best practices and mitigation strategies (ES ≥ 0.54, p < .0001). Qualitative comments supported this increase.
Healthcare providers: despite no significant change in self-reported levels of knowledge and confidence, they commented that the educational activity could help in their assessments of environmental triggers and could provide recommendations of strategies to incorporate into care plans.
The virtual trigger room was found to be a feasible educational activity that enhanced learning, increased awareness of environmental triggers and could be helpful for direct application into clinical practice.
Since this was a proof of concept study, limitations included a small sample of healthcare providers and inclusion of only an immediate post-evaluation of the educational tool. We plan to expand our subject groups to include caregivers of persons with dementia (both paid and unpaid) and a larger number of healthcare providers to validate the initial results. We also plan to build a version that occurs in a long-term care setting with illustrations and videos, as triggers for responsive behaviours are prevalent in this environment. Future evaluations will also include the evaluation of impact/application of learning approximately two to three months post activity.
The authors would like to thank Dr. David Conn for his assistance with reviewing and revising the triggers and strategies and for his overall support of this project. The authors would also like to thank Candice Yiu for her assistance with student recruitment.
All authors have made a significant contribution to the paper.
This project was supported by a grant from the Ontario Ministry of Health and Long-Term Care, Academic Health Science Centre Alternate Funding Plan Innovation Fund.
Data available from authors upon reasonable request.
This project has research approval from the Research Ethics Board at Baycrest, REB#20–32. All research participants signed an online informed consent form.
The authors declare no conflict of interest.
1.
2.
3.
4.
5.
 The virtual trigger room – a proof of concept
The virtual trigger room – a proof of concept
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets