
Aspiration of gastric contents remains the commonest cause of death during anaesthesia, accounting for 50% of deaths and occurring more frequently than cannot intubate, cannot oxygenate (CICO) events [1]. Despite this, training for CICO is ubiquitous while rehearsal of aspiration management is rare. Soiled airway simulation has been shown to reduce the time to intubation with less volume entering the lungs, a factor known to correlate with the severity of aspiration [2]. Initially developed by Dr DuCanto, high-fidelity vomit simulators have existed since 2014 however cost (£1,595) precludes their widespread use. Low-cost models have since been described, however, the materials are sourced from hardware stores, relatively expensive, require skills to construct, utilise noisy pumps, and some even require electrical safety considerations [3]. We aimed to improve access to aspiration training by designing an aspiration simulator that is easy to construct and low-cost.
Employing an iterative design process we created an aspiration simulator using materials readily available in the operating theatre. The final model requires an intubatable manikin with an oesophagus, such as the Laerdal Airway Management TrainerTM. The oesophagus is intubated distally with a shortened size 9.0 cuffed endotracheal tube (acting as both a conduit and seal), which is then connected to a shortened bladder irrigation set and two 3-litre bags containing simulated regurgitation (made from propofol, water, and green food colouring), elevated and manually pressurised to 300 mmHg (Figure 1, upper left).

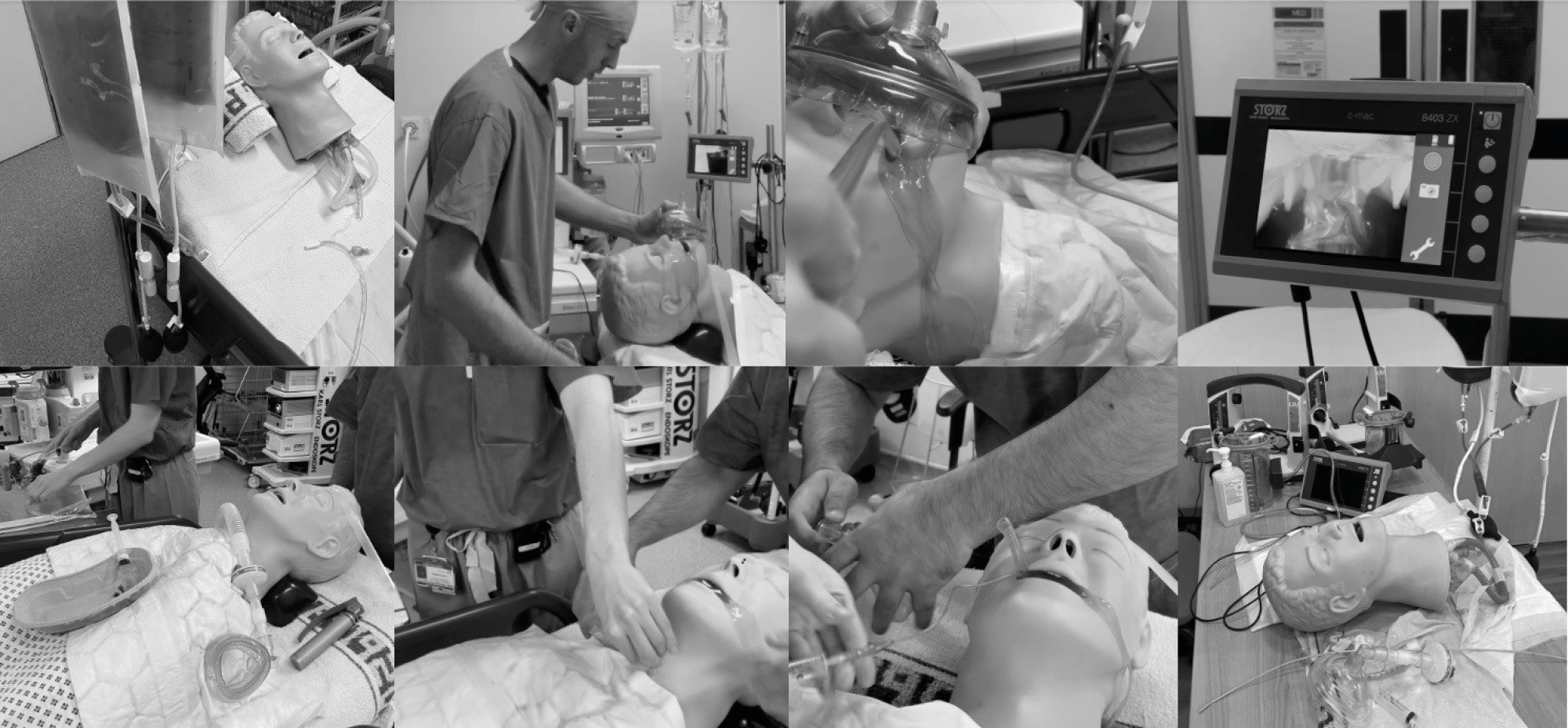
The setup silently produces a titratable flow of up to 250 ml per minute, sufficient to flood the oropharynx within 30 seconds. The simulation itself can be set up in under 10 minutes, used several times before requiring refilling, and is easily transported between theatres as a part-task trainer or concealed for a multi-disciplinary simulation (Figure 1, bottom left). All parts are reusable and the total cost equals £9.90 (excluding the manikin, which is undamaged). Our simulator was tested on a cohort of 16 middle-grade anaesthetic trainees and its performance was evaluated using pre and post-course questionnaires (scale 0–10). All successfully intubated the simulator. Average user-rating scores for realism were 8.4/10 while confidence in managing soiled airways improved from 6.2/10 to 8.9/10 after exposure to the simulation.
Soiled airway simulation can be simple and affordable, creating a realistic environment to practise the unique skills necessary to manage this important yet under-rehearsed cause of death during anaesthesia.
1. Cook T, Woodall N, Frerk C. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia †. British Journal of Anaesthesia. 2011;106(5):617–631
2. Jensen M, Louka A, Barmaan B. Effect of Suction Assisted Laryngoscopy Airway Decontamination (SALAD) Training on Intubation Quality Metrics. Air Medical Journal. 2019;38(5):325.
3. Sampson C, Pauly J, Horner J. Low-cost Portable Suction-Assisted Laryngoscopy Airway Decontamination (SALAD) Simulator for Dynamic Emesis. Journal of Education and Teaching in Emergency Medicine. 2019;4(2).
 Creating an easy to construct, low-cost aspiration simulator for airway training
Creating an easy to construct, low-cost aspiration simulator for airway training
 Facebook
Facebook
 Twitter
Twitter
 Linkedin
Linkedin
 Whatsapp
Whatsapp
 Tweets
Tweets